Canadian Journal of Emergency Medicine ( IF 2.0 ) Pub Date : 2022-09-21 , DOI: 10.1007/s43678-022-00355-4 Aisha Moustapha 1 , Alicia C Mah 1 , Lauren Roberts 2 , Andrew Leach 2 , Glenda Kaban 3 , Rodney Zimmermann 4 , Jay Shavadia 5 , Jason Orvold 5 , Prosanta Mondal 6 , Lynsey J Martin 2
|
Purpose
Current guidelines recommend hospital admission for patients who present to the emergency department (ED) with chest pain and are scored as intermediate risk for adverse outcomes based on the HEART score. While hospital admission for these patients allows for timely investigation and treatment, it is a resource-intensive process. This study examines whether intermediate HEART score patients can be safely managed on an outpatient basis through rapid access chest pain clinics.
Methods
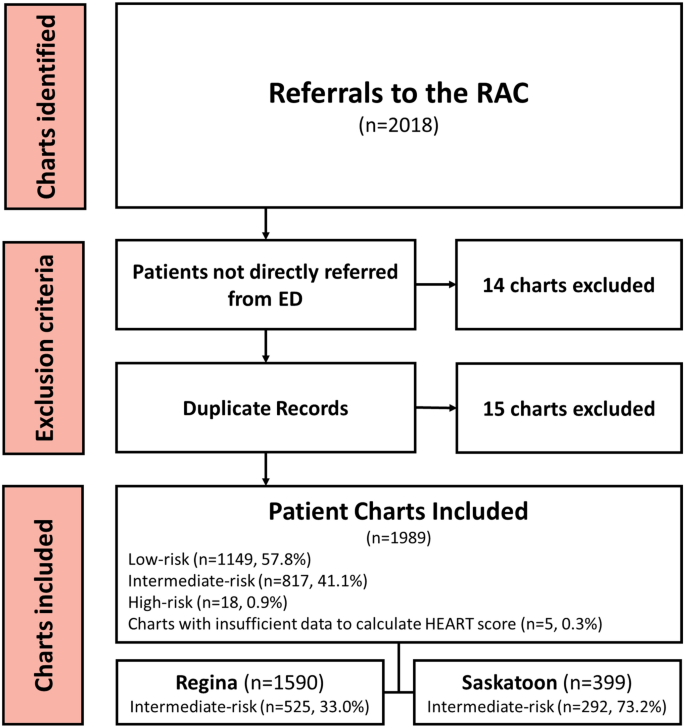
This retrospective observational study included all ED chest pain patients referred to rapid access clinics from January 2018 to April 2020 in Regina and Saskatoon, Saskatchewan. ED physician HEART scores were used in lieu of reviewer HEART scores when available. The primary outcome was the rate of major adverse coronary events (MACE), a composite measure of death, acute coronary syndrome, stroke, coronary angiography, and revascularization at 6 weeks in intermediate-risk patients. Secondary outcomes were the type of MACE, rate of MACE before rapid access clinic appointment and the most predictive component of the HEART score.
Results
There were 1989 ED referrals, of which 817 were for intermediate-risk patients. 9.3% of intermediate-risk patients had a MACE at 6 weeks. MACE occurred before rapid access clinic follow-up in 1.1% of intermediate-risk patients, with coronary angiography being the most common MACE. Excluding coronary angiography, the risk of MACE before rapid access clinic follow-up was 0.7% in intermediate-risk patients. Components of the HEART score most predictive of MACE were troponin (OR 11.0, 95% CI: 3.7–32.3) and history (5.3, 95% CI: 2.4–11.8).
Conclusion
This study demonstrates that rapid access clinics are likely a safe alternative to admission for intermediate-risk chest pain patients and could reduce costly inpatient admissions for chest pain. With angiography excluded, MACE rates were well below the American College of Emergency Physicians cited 2% threshold.
中文翻译:
具有中间 HEART 评分的 ED 胸痛患者可以作为门诊患者进行管理吗?
目的
目前的指南建议因胸痛就诊于急诊科 (ED) 且根据 HEART 评分被评为不良结局中等风险的患者入院。虽然让这些患者入院可以进行及时的调查和治疗,但这是一个资源密集型过程。本研究检查是否可以通过快速访问胸痛诊所在门诊病人的基础上安全地管理中间 HEART 评分患者。
方法
这项回顾性观察研究包括 2018 年 1 月至 2020 年 4 月在萨斯喀彻温省里贾纳和萨斯卡通转诊到快速通道诊所的所有 ED 胸痛患者。ED 医师 HEART 分数可用时代替审阅者 HEART 分数。主要结局是主要不良冠状动脉事件 (MACE) 的发生率,这是中度风险患者 6 周时死亡、急性冠状动脉综合征、卒中、冠状动脉造影和血运重建的综合指标。次要结果是 MACE 的类型、快速访问门诊预约前 MACE 的发生率和 HEART 评分中最具预测性的组成部分。
结果
有 1989 例急诊转诊,其中 817 例是针对中危患者。9.3% 的中危患者在 6 周时发生 MACE。MACE 发生在 1.1% 的中危患者的快速访问门诊随访之前,冠状动脉造影是最常见的 MACE。排除冠状动脉造影,中危患者在快速访问门诊随访前发生 MACE 的风险为 0.7%。最能预测 MACE 的 HEART 评分成分是肌钙蛋白(OR 11.0,95% CI:3.7-32.3)和病史(5.3,95% CI:2.4-11.8)。
结论
这项研究表明,快速就诊诊所可能是中危胸痛患者入院的安全替代方案,并且可以减少因胸痛而住院的昂贵费用。排除血管造影,MACE 发生率远低于美国急诊医师学会引用的 2% 阈值。








































 京公网安备 11010802027423号
京公网安备 11010802027423号