Pediatric Nephrology ( IF 2.6 ) Pub Date : 2022-08-02 , DOI: 10.1007/s00467-022-05651-w Nori J L Smeets 1, 2 , Esther M M Teunissen 1 , Kim van der Velden 1 , Maurice J P van der Burgh 1 , Demi E Linders 1 , Elodie Teesselink 1 , Dirk-Jan A R Moes 3 , Camilla Tøndel 4 , Rob Ter Heine 5 , Arno van Heijst 6 , Michiel F Schreuder 7 , Saskia N de Wildt 1, 2
|
Background
Acute kidney injury (AKI) and augmented renal clearance (ARC), both alterations of the glomerular filtration rate (GFR), are prevalent in critically ill children and neonates. AKI and ARC prevalence estimates are based on estimation of GFR (eGFR) using serum creatinine (SCr), which is known to be inaccurate. We aimed to test our hypothesis that AKI prevalence will be higher and ARC prevalence will be lower in critically ill children when using iohexol-based measured GFR (mGFR), rather than using eGFR. Additionally, we aimed to investigate the performance of different SCr-based eGFR methods.
Methods
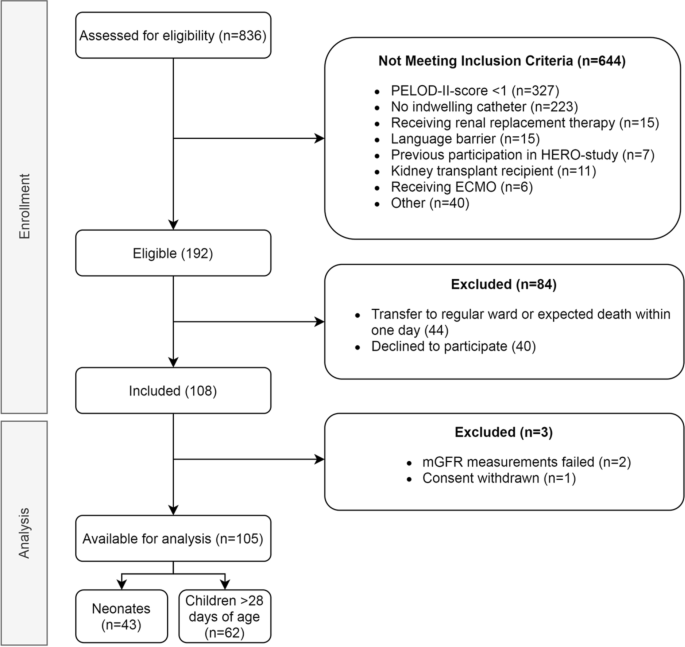
In this single-center prospective study, critically ill term-born neonates and children were included. mGFR was calculated using a plasma disappearance curve after parenteral administration of iohexol. AKI diagnosis was based on the KDIGO criteria, SCr-based eGFR, and creatinine clearance (CrCL). Differences between eGFR and mGFR were determined using Wilcoxon signed-rank tests and by calculating bias and accuracy (percentage of eGFR values within 30% of mGFR values).
Results
One hundred five children, including 43 neonates, were included. AKI prevalence was higher based on mGFR (48%), than with KDIGO or eGFR (11–40%). ARC prevalence was lower with mGFR (24%) compared to eGFR (38–51%). eGFR equations significantly overestimated mGFR (60–71 versus 41 ml/min/1.73 m2, p < 0.001–0.002). Accuracy was highest with eGFR equations based on age- and sex-dependent equations (up to 59%).
Conclusion
Iohexol-based AKI prevalence was higher and ARC prevalence lower compared to standard SCr-based eGFR methods. Age- and sex-dependent equations for eGFR (eGFR-Smeets for neonates and eGFR-Pierce for children) best approached measured GFR and should preferably be used to optimize diagnosis of AKI and ARC in this population.
Graphical Abstract
A higher resolution version of the Graphical abstract is available as Supplementary information
中文翻译:
危重新生儿和儿童的肾小球滤过率:基于肌酐的估计与基于碘海醇的测量
背景
急性肾损伤 (AKI) 和肾清除率增加 (ARC) 这两种肾小球滤过率 (GFR) 的改变在危重儿童和新生儿中很普遍。AKI 和 ARC 患病率估计是基于使用血清肌酐 (SCr) 对 GFR (eGFR) 的估计,这被认为是不准确的。我们的目的是检验我们的假设,即当使用基于碘海醇的测量 GFR (mGFR) 而不是使用 eGFR 时,危重儿童的 AKI 患病率会更高,ARC 患病率会更低。此外,我们旨在研究不同基于 SCr 的 eGFR 方法的性能。
方法
在这项单中心前瞻性研究中,包括危重的足月新生儿和儿童。mGFR 是在胃肠外给药碘海醇后使用血浆消失曲线计算的。AKI 诊断基于 KDIGO 标准、基于 SCr 的 eGFR 和肌酐清除率 (CrCL)。eGFR 和 mGFR 之间的差异是使用 Wilcoxon 符号秩检验和计算偏差和准确性(eGFR 值在 mGFR 值的 30% 以内的百分比)来确定的。
结果
包括 43 名新生儿在内的 105 名儿童被纳入。基于 mGFR (48%) 的 AKI 患病率高于 KDIGO 或 eGFR (11-40%)。与 eGFR (38–51%) 相比,mGFR (24%) 的 ARC 患病率较低。eGFR 方程显着高估了 mGFR(60–71 对比 41 ml/min/1.73 m 2,p < 0.001–0.002)。基于年龄和性别相关方程的 eGFR 方程的准确性最高(高达 59%)。
结论
与标准的基于 SCr 的 eGFR 方法相比,基于碘海醇的 AKI 患病率更高,ARC 患病率更低。eGFR 的年龄和性别依赖方程(新生儿的 eGFR-Smeets 和儿童的 eGFR-Pierce)最接近测量的 GFR,应该优先用于优化该人群中 AKI 和 ARC 的诊断。
图形概要
图形摘要的更高分辨率版本可作为补充信息使用








































 京公网安备 11010802027423号
京公网安备 11010802027423号