Journal of Interventional Cardiac Electrophysiology ( IF 2.1 ) Pub Date : 2021-11-25 , DOI: 10.1007/s10840-021-01073-0 Nicolas Dognin 1 , Erwan Salaun 1 , Catherine Champagne 1 , Guillaume Domain 1 , Gilles O’Hara 1 , François Philippon 1 , Jean-Michel Paradis 1 , Laurent Faroux 1 , Jonathan Beaudoin 1 , Kim O’Connor 1 , Mathieu Bernier 1 , Josep Rodés-Cabau 1 , Jean Champagne 1
|
Background or purpose
We report our single-center experience with percutaneous left atrial appendage closure (LAAC) in patients with non-valvular atrial fibrillation (NVAF) and primary hemostasis disorders (HD).
Methods
Consecutive patients with primary HD who underwent a percutaneous LAAC were included. Baseline characteristics, procedural data, and clinical outcomes were prospectively collected and compared with the overall LAAC cohort without HD.
Results
Since 2013, among 229 LAAC, 17 patients (7%) had a primary HD: thrombocytopenia (n = 5), myelodysplastic syndrome (n = 6), von Willebrand syndrome (n = 4), type A hemophilia (n = 1), and dysfibrinogenemia (n = 1). The HD population’s age ranged from 61 to 87 years, and the median CHA2DS2VASc was 5. Periprocedural plasmatic management was required in 47% of patients. The immediate LAAC implantation success rate was 100%. Patients received a direct oral anticoagulant (DOA) (n = 9), dual antiplatelet (n = 6), aspirin (n = 1), or no therapy (n = 1) during the first six postoperative weeks, followed with single antiplatelet (n = 16) or no therapy (n = 1) during lifelong. After 20 months, the technical success rate and procedural success rate were 100% and 94%. Zero device-/procedure-related complication and only one life-threatening bleeding occurred. Compared to patients without HD (n = 212), a baseline history of bleeding was less frequent (53% vs 91%, p < 0.001), and more patients received a perioperative blood transfusion (47% vs 4%, p < 0.001) in the HD group. The efficacy and safety outcomes did not differ between HD and non-HD cohorts.
Conclusions
Percutaneous LAAC in primary HD carriers appeared as safe and as effective as in overall LAAC population for stroke and bleeding prevention at midterm follow-up.
Graphical abstract
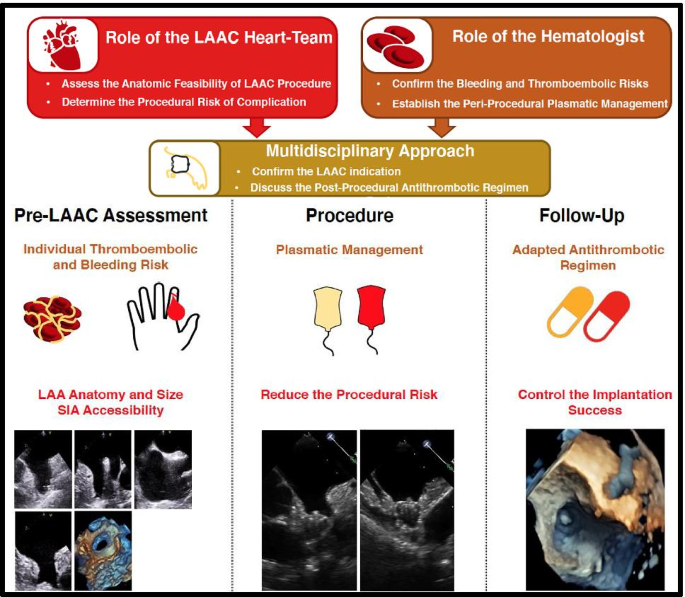
Percutaneous left atrial appendage closure in patients with atrial fibrillation and primary hemostasis disorders. The percutaneous LAAC in primary hemostasis disorders and AF carriers requires a multidisciplinary approach. Cardiologist, anesthesiologist, and hematologist discussion is a cornerstone to assess anticoagulant contraindication, LAAC feasibility, periprocedural management, and follow-up (high). This multidisciplinary care is illustrated by the case of a 61-year-old male with hemophilia type A and recurrent hemarthrosis. Pre-LAAC assessment confirmed procedural indication and cactus LAA anatomy (left). After plasmatic management with factor VIII infusion, a WATCHMAN™ no. 21 was successfully implanted (middle). During follow-up, without antithrombotic regime, no ischemic or hemorrhagic complication occurred (right). LAA, left atrial appendage; LAAC, left atrial appendage closure; TEE, transesophageal echocardiography. Percutaneous LAAC in primary HD carriers appeared as safe and as effective as in overall LAAC population for stroke and bleeding prevention at midterm follow-up.
中文翻译:
原发性止血障碍和心房颤动患者经皮左心耳封堵术
背景或目的
我们报告了我们在非瓣膜性心房颤动 (NVAF) 和原发性止血障碍 (HD) 患者中经皮左心耳封堵术 (LAAC) 的单中心经验。
方法
包括接受经皮 LAAC 的连续原发性 HD 患者。前瞻性收集基线特征、程序数据和临床结果,并与没有 HD 的整个 LAAC 队列进行比较。
结果
自 2013 年以来,在 229 名 LAAC 中,17 名患者 (7%) 患有原发性 HD:血小板减少症 ( n = 5)、骨髓增生异常综合征 ( n = 6)、von Willebrand 综合征 ( n = 4)、A 型血友病 ( n = 1)和异常纤维蛋白原血症 ( n = 1)。HD 人群的年龄范围为 61 至 87 岁,CHA 2 DS 2 VASc的中位数为 5。47% 的患者需要围手术期血浆治疗。即刻 LAAC 植入成功率为 100%。患者接受直接口服抗凝剂 (DOA) ( n = 9)、双重抗血小板 ( n = 6)、阿司匹林 ( n = 1) 或不接受治疗 ( n = 1) 在术后前六周内,随后 终生接受单一抗血小板 ( n = 16) 或不治疗 ( n = 1)。20个月后,技术成功率和程序成功率分别为100%和94%。与设备/程序相关的并发症为零,并且仅发生了一次危及生命的出血。与没有 HD 的患者 ( n = 212) 相比,基线出血史较少(53% 对 91%,p < 0.001),更多的患者接受围手术期输血(47% 对 4%,p < 0.001)在高清组。HD 和非 HD 队列的疗效和安全性结果没有差异。
结论
在中期随访中,原发性 HD 携带者的经皮 LAAC 与整个 LAAC 人群一样安全有效,可预防卒中和出血。
图形概要
房颤和原发性止血障碍患者的经皮左心耳封堵术。原发性止血障碍和 AF 携带者的经皮 LAAC 需要多学科方法。心脏科医师、麻醉科医师和血液科医师的讨论是评估抗凝禁忌症、LAAC 可行性、围手术期管理和随访的基石(高)。一名患有 A 型血友病和关节积血的 61 岁男性的案例说明了这种多学科护理。LAAC 前评估确认了手术适应症和仙人掌 LAA 解剖结构(左)。输注凝血因子 VIII 后,WATCHMAN™ 没有。21 成功植入(中). 在随访期间,在没有抗血栓治疗的情况下,没有发生缺血性或出血性并发症(右)。LAA,左心耳;LAAC,左心耳闭合;TEE,经食道超声心动图。在中期随访中,原发性 HD 携带者的经皮 LAAC 与整个 LAAC 人群一样安全有效,可预防卒中和出血。










































 京公网安备 11010802027423号
京公网安备 11010802027423号