JACC: Heart Failure ( IF 10.3 ) Pub Date : 2021-05-12 , DOI: 10.1016/j.jchf.2021.02.011 Michael A Fuery 1 , Fouad Chouairi 2 , James L Januzzi 3 , Gordon W Moe 4 , Cesar Caraballo 5 , Megan McCullough 1 , P Elliott Miller 2 , Samuel W Reinhardt 2 , Katherine Clark 2 , Andrew Oseran 3 , Aidan Milner 1 , Justin Pacor 1 , Peter A Kahn 1 , Avinainder Singh 1 , Neal Ravindra 6 , Avirup Guha 7 , Lina Vadlamani 2 , Neeti S Kulkarni 8 , Mona Fiuzat 9 , G Michael Felker 9 , Christopher M O'Connor 10 , Tariq Ahmad 11 , Justin Ezekowitz 12 , Nihar R Desai 11
|
Objectives
The aim of this study was to examine patterns of care and clinical outcomes among patients with heart failure with reduced ejection fraction (HFrEF) in the United States and Canada.
Background
In the GUIDE-IT (Guiding Evidence Based Therapy Using Biomarker Intensified Treatment) trial, the use of N-terminal pro–B-type natriuretic peptide–guided titration of guideline-directed medical therapy (GDMT) was compared with usual care alone for patients with HFrEF in the United States and Canada. It remains unknown whether the country of enrollment had an impact on outcomes or GDMT use.
Methods
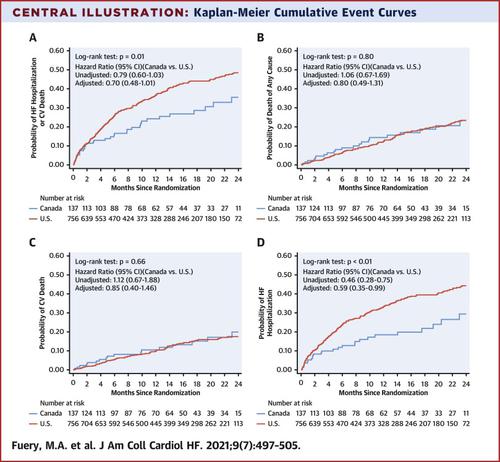
A total of 894 patients at 45 sites across the United States and Canada with HFrEF (ejection fraction ≤40%) were enrolled in the trial. Kaplan-Meier survival estimates stratified by country of enrollment were developed for the trial outcomes, and log-rank testing was compared between the groups. GDMT use and titration were also compared.
Results
U.S. patients were more likely to be younger, to be Black, to have higher body mass index, and to have histories of defibrillator placement or sleep apnea. Use of β-blockers was significantly higher in Canada at baseline (99.3% vs. 94.0%; p = 0.01) and 6 months (99.0% vs. 94.1%; p = 0.04), and use of mineralocorticoid receptor antagonists was higher in Canada at 6 months (68.3% vs. 55.1%; p = 0.01). Canadian patients were less likely to experience the primary study endpoint (hazard ratio [HR]: 0.65; 95% confidence interval [CI]: 0.45 to 0.93; p = 0.01) due to decreased rates of HF hospitalization (HR: 0.57; 95% CI: 0.38 to 0.86; p = 0.003). The differences in outcomes were driven by increased heart failure hospitalization among U.S. Black patients.
Conclusions
In GUIDE-IT, patients with HFrEF in Canada were significantly less likely to be hospitalized for heart failure. Differences in GDMT use, along with differences in sociodemographics and care delivery structures, may contribute to these differences, highlighting the importance of increasing diversity in clinical trials. (Guiding Evidence Based Therapy Using Biomarker Intensified Treatment [GUIDE-IT]; NCT01685840)
中文翻译:
心力衰竭患者指南指导药物治疗和结果的国家间差异
目标
本研究的目的是检查美国和加拿大射血分数降低的心力衰竭 (HFrEF) 患者的护理模式和临床结果。
背景
在 GUIDE-IT(使用生物标志物强化治疗指导循证治疗)试验中,将使用 N 端 B 型利钠肽前体引导滴定的指南指导药物治疗 (GDMT) 与单独对患者进行常规治疗进行了比较在美国和加拿大使用 HFrEF。目前尚不清楚注册国家是否对结果或 GDMT 使用产生影响。
方法
在美国和加拿大的 45 个地点共有 894 名 HFrEF(射血分数≤40%)患者参加了试验。为试验结果制定了按入组国家分层的 Kaplan-Meier 生存估计值,并比较了组间的时序检验。还比较了 GDMT 的使用和滴定。
结果
美国患者更年轻、更可能是黑人、体重指数更高,以及有除颤器放置或睡眠呼吸暂停病史。在基线(99.3% vs. 94.0%;p = 0.01)和 6 个月(99.0% vs. 94.1%;p = 0.04)时,加拿大的 β 受体阻滞剂使用率显着增加,加拿大盐皮质激素受体拮抗剂的使用率更高6 个月时(68.3% 对 55.1%;p = 0.01)。由于 HF 住院率降低(HR:0.57;95% CI:0.38 至 0.86;p = 0.003)。结果的差异是由于美国黑人患者心力衰竭住院率增加所致。
结论
在 GUIDE-IT 中,加拿大 HFrEF 患者因心力衰竭住院的可能性显着降低。GDMT 使用的差异,以及社会人口统计学和护理提供结构的差异,可能导致这些差异,突出了增加临床试验多样性的重要性。(使用生物标志物强化治疗指导循证治疗 [GUIDE-IT];NCT01685840)










































 京公网安备 11010802027423号
京公网安备 11010802027423号