Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Variability in the use of pulse oximeters with children in Kenyan hospitals: A mixed-methods analysis.
PLOS Medicine ( IF 15.8 ) Pub Date : 2019-12-31 , DOI: 10.1371/journal.pmed.1002987 Abigail J Enoch 1 , Mike English 2, 3 , , Gerald McGivern 4 , Sasha Shepperd 5
PLOS Medicine ( IF 15.8 ) Pub Date : 2019-12-31 , DOI: 10.1371/journal.pmed.1002987 Abigail J Enoch 1 , Mike English 2, 3 , , Gerald McGivern 4 , Sasha Shepperd 5
Affiliation
|
BACKGROUND
Pulse oximetry, a relatively inexpensive technology, has the potential to improve health outcomes by reducing incorrect diagnoses and supporting appropriate treatment decisions. There is evidence that in low- and middle-income countries, even when available, widespread uptake of pulse oximeters has not occurred, and little research has examined why. We sought to determine when and with which children pulse oximeters are used in Kenyan hospitals, how pulse oximeter use impacts treatment provision, and the barriers to pulse oximeter use.
METHODS AND FINDINGS
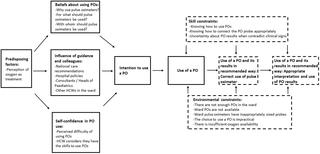
We analyzed admissions data recorded through Kenya's Clinical Information Network (CIN) between September 2013 and February 2016. We carried out multiple imputation and generated multivariable regression models in R. We also conducted interviews with 30 healthcare workers and staff from 14 Kenyan hospitals to examine pulse oximetry adoption. We adapted the Integrative Model of Behavioural Prediction to link the results from the multivariable regression analyses to the qualitative findings. We included 27,906 child admissions from 7 hospitals in the quantitative analyses. The median age of the children was 1 year, and 55% were male. Three-quarters had a fever, over half had a cough; other symptoms/signs were difficulty breathing (34%), difficulty feeding (34%), and indrawing (32%). The most common diagnoses were pneumonia, diarrhea, and malaria: 45%, 35%, and 28% of children, respectively, had these diagnoses. Half of the children obtained a pulse oximeter reading, and of these, 10% had an oxygen saturation level below 90%. Children were more likely to receive a pulse oximeter reading if they were not alert (odds ratio [OR]: 1.30, 95% confidence interval (CI): 1.09, 1.55, p = 0.003), had chest indrawing (OR: 1.28, 95% CI: 1.17, 1.40, p < 0.001), or a very high respiratory rate (OR: 1.27, 95% CI: 1.13, 1.43, p < 0.001), as were children admitted to certain hospitals, at later time periods, and when a Paediatric Admission Record (PAR) was used (OR PAR used compared with PAR not present: 2.41, 95% CI: 1.98, 2.94, p < 0.001). Children were more likely to be prescribed oxygen if a pulse oximeter reading was obtained (OR: 1.42, 95% CI:1.25, 1.62, p < 0.001) and if this reading was below 90% (OR: 3.29, 95% CI: 2.82, 3.84, p < 0.001). The interviews indicated that the main barriers to pulse oximeter use are inadequate supply, broken pulse oximeters, and insufficient training on how, when, and why to use pulse oximeters and interpret their results. According to the interviews, variation in pulse oximeter use between hospitals is because of differences in pulse oximeter availability and the leadership of senior doctors in advocating for pulse oximeter use, whereas variation within hospitals over time is due to repair delays. Pulse oximeter use increased over time, likely because of the CIN's feedback to hospitals. When pulse oximeters are used, they are sometimes used incorrectly and some healthcare workers lack confidence in readings that contradict clinical signs. The main limitations of the study are that children with high levels of missing data were not excluded, interview participants might not have been representative, and the interviews did not enable a detailed exploration of differences between counties or across senior management groups.
CONCLUSIONS
There remain major challenges to implementing pulse oximetry-a cheap, decades old technology-into routine care in Kenya. Implementation requires efficient and transparent procurement and repair systems to ensure adequate availability. Periodic training, structured clinical records that include prompts, the promotion of pulse oximetry by senior doctors, and monitoring and feedback might also support pulse oximeter use. Our findings can inform strategies to support the use of pulse oximeters to guide prompt and effective treatment, in line with the Sustainable Development Goals. Without effective implementation, the potential benefits of pulse oximeters and possible hospital cost-savings by targeting oxygen therapy might not be realized.
中文翻译:

肯尼亚医院儿童脉搏血氧仪使用的可变性:混合方法分析。
背景技术脉搏血氧仪是一种相对便宜的技术,具有通过减少错误的诊断并支持适当的治疗决定来改善健康结果的潜力。有证据表明,即使在低收入和中等收入国家,脉搏血氧仪也没有得到广泛的吸收,很少有研究探讨其原因。我们试图确定在肯尼亚医院何时以及与哪些儿童一起使用脉搏血氧仪,脉搏血氧仪的使用如何影响治疗提供,以及脉搏血氧仪使用的障碍。方法和结果我们分析了2013年9月至2016年2月间通过肯尼亚临床信息网络(CIN)记录的入院数据。我们在R中进行了多重估算并生成了多变量回归模型。我们还采访了肯尼亚14家医院的30名医护人员和工作人员,以检查脉搏血氧饱和度的采用情况。我们调整了行为预测的集成模型,以将多变量回归分析的结果与定性发现联系起来。在定量分析中,我们纳入了来自7家医院的27906名儿童入院。儿童的中位年龄为1岁,其中55%为男性。四分之三的人发烧,一半以上的人咳嗽。其他症状/体征包括呼吸困难(34%),进食困难(34%)和吸食困难(32%)。最常见的诊断是肺炎,腹泻和疟疾:分别有45%,35%和28%的儿童患有这些诊断。一半的孩子获得了脉搏血氧仪的读数,其中有10%的孩子的血氧饱和度低于90%。如果儿童不警觉,他们更有可能接受脉搏血氧仪读数(优势比[OR]:1.30,95%置信区间(CI):1.09、1.55,p = 0.003),并且有胸部抽搐(OR:1.28、95) CI的百分比:1.17、1.40,p <0.001)或很高的呼吸频率(OR:1.27,95%CI:1.13、1.43,p <0.001)。当使用儿科入院记录(PAR)时(使用的PAR与不存在的PAR相比:2.41、95%CI:1.98、2.94,p <0.001)。如果获得脉搏血氧仪读数(OR:1.42,95%CI:1.25,1.62,p <0.001),并且读数低于90%(OR:3.29,95%CI:2.82),则儿童更容易被处方服用氧气。 ,3.84,p <0.001)。访谈表明,使用脉搏血氧仪的主要障碍是供应不足,脉搏血氧仪损坏,对如何,何时以及为什么使用脉搏血氧仪并解释其结果的培训不足。根据访谈,医院之间脉搏血氧仪使用的变化是由于脉搏血氧仪可用性的差异以及高级医生在倡导脉搏血氧仪使用方面的领导,而医院内部随时间的变化是由于维修延迟。脉搏血氧仪的使用随着时间的推移而增加,这可能是由于CIN向医院提供了反馈。使用脉搏血氧仪时,有时会使用不正确,并且某些医护人员对与临床体征相矛盾的读数缺乏信心。该研究的主要局限性是没有排除那些缺少大量数据的孩子,访谈参与者可能没有代表性,采访无法详细探究县之间或高层管理人员之间的差异。结论在肯尼亚,将脉搏血氧仪(一种便宜的,已有数十年历史的技术)实施到日常护理中仍然存在重大挑战。实施需要高效,透明的采购和维修系统,以确保足够的可用性。定期培训,结构化的临床记录(包括提示),高级医生对脉搏血氧仪的促进以及监测和反馈也可能支持脉搏血氧仪的使用。我们的发现可以为根据可持续发展目标支持脉搏血氧仪指导快速有效治疗提供依据的策略。没有有效的实施,
更新日期:2020-01-14
中文翻译:
肯尼亚医院儿童脉搏血氧仪使用的可变性:混合方法分析。
背景技术脉搏血氧仪是一种相对便宜的技术,具有通过减少错误的诊断并支持适当的治疗决定来改善健康结果的潜力。有证据表明,即使在低收入和中等收入国家,脉搏血氧仪也没有得到广泛的吸收,很少有研究探讨其原因。我们试图确定在肯尼亚医院何时以及与哪些儿童一起使用脉搏血氧仪,脉搏血氧仪的使用如何影响治疗提供,以及脉搏血氧仪使用的障碍。方法和结果我们分析了2013年9月至2016年2月间通过肯尼亚临床信息网络(CIN)记录的入院数据。我们在R中进行了多重估算并生成了多变量回归模型。我们还采访了肯尼亚14家医院的30名医护人员和工作人员,以检查脉搏血氧饱和度的采用情况。我们调整了行为预测的集成模型,以将多变量回归分析的结果与定性发现联系起来。在定量分析中,我们纳入了来自7家医院的27906名儿童入院。儿童的中位年龄为1岁,其中55%为男性。四分之三的人发烧,一半以上的人咳嗽。其他症状/体征包括呼吸困难(34%),进食困难(34%)和吸食困难(32%)。最常见的诊断是肺炎,腹泻和疟疾:分别有45%,35%和28%的儿童患有这些诊断。一半的孩子获得了脉搏血氧仪的读数,其中有10%的孩子的血氧饱和度低于90%。如果儿童不警觉,他们更有可能接受脉搏血氧仪读数(优势比[OR]:1.30,95%置信区间(CI):1.09、1.55,p = 0.003),并且有胸部抽搐(OR:1.28、95) CI的百分比:1.17、1.40,p <0.001)或很高的呼吸频率(OR:1.27,95%CI:1.13、1.43,p <0.001)。当使用儿科入院记录(PAR)时(使用的PAR与不存在的PAR相比:2.41、95%CI:1.98、2.94,p <0.001)。如果获得脉搏血氧仪读数(OR:1.42,95%CI:1.25,1.62,p <0.001),并且读数低于90%(OR:3.29,95%CI:2.82),则儿童更容易被处方服用氧气。 ,3.84,p <0.001)。访谈表明,使用脉搏血氧仪的主要障碍是供应不足,脉搏血氧仪损坏,对如何,何时以及为什么使用脉搏血氧仪并解释其结果的培训不足。根据访谈,医院之间脉搏血氧仪使用的变化是由于脉搏血氧仪可用性的差异以及高级医生在倡导脉搏血氧仪使用方面的领导,而医院内部随时间的变化是由于维修延迟。脉搏血氧仪的使用随着时间的推移而增加,这可能是由于CIN向医院提供了反馈。使用脉搏血氧仪时,有时会使用不正确,并且某些医护人员对与临床体征相矛盾的读数缺乏信心。该研究的主要局限性是没有排除那些缺少大量数据的孩子,访谈参与者可能没有代表性,采访无法详细探究县之间或高层管理人员之间的差异。结论在肯尼亚,将脉搏血氧仪(一种便宜的,已有数十年历史的技术)实施到日常护理中仍然存在重大挑战。实施需要高效,透明的采购和维修系统,以确保足够的可用性。定期培训,结构化的临床记录(包括提示),高级医生对脉搏血氧仪的促进以及监测和反馈也可能支持脉搏血氧仪的使用。我们的发现可以为根据可持续发展目标支持脉搏血氧仪指导快速有效治疗提供依据的策略。没有有效的实施,


























 京公网安备 11010802027423号
京公网安备 11010802027423号