Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Polygenic risk-tailored screening for prostate cancer: A benefit-harm and cost-effectiveness modelling study.
PLOS Medicine ( IF 10.5 ) Pub Date : 2019-12-20 , DOI: 10.1371/journal.pmed.1002998 Tom Callender 1 , Mark Emberton 2 , Steve Morris 1 , Ros Eeles 3 , Zsofia Kote-Jarai 3 , Paul D P Pharoah 4 , Nora Pashayan 1
PLOS Medicine ( IF 10.5 ) Pub Date : 2019-12-20 , DOI: 10.1371/journal.pmed.1002998 Tom Callender 1 , Mark Emberton 2 , Steve Morris 1 , Ros Eeles 3 , Zsofia Kote-Jarai 3 , Paul D P Pharoah 4 , Nora Pashayan 1
Affiliation
|
BACKGROUND
The United States Preventive Services Task Force supports individualised decision-making for prostate-specific antigen (PSA)-based screening in men aged 55-69. Knowing how the potential benefits and harms of screening vary by an individual's risk of developing prostate cancer could inform decision-making about screening at both an individual and population level. This modelling study examined the benefit-harm tradeoffs and the cost-effectiveness of a risk-tailored screening programme compared to age-based and no screening.
METHODS AND FINDINGS
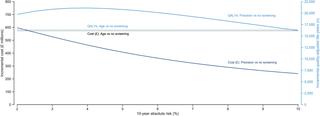
A life-table model, projecting age-specific prostate cancer incidence and mortality, was developed of a hypothetical cohort of 4.48 million men in England aged 55 to 69 years with follow-up to age 90. Risk thresholds were based on age and polygenic profile. We compared no screening, age-based screening (quadrennial PSA testing from 55 to 69), and risk-tailored screening (men aged 55 to 69 years with a 10-year absolute risk greater than a threshold receive quadrennial PSA testing from the age they reach the risk threshold). The analysis was undertaken from the health service perspective, including direct costs borne by the health system for risk assessment, screening, diagnosis, and treatment. We used probabilistic sensitivity analyses to account for parameter uncertainty and discounted future costs and benefits at 3.5% per year. Our analysis should be considered cautiously in light of limitations related to our model's cohort-based structure and the uncertainty of input parameters in mathematical models. Compared to no screening over 35 years follow-up, age-based screening prevented the most deaths from prostate cancer (39,272, 95% uncertainty interval [UI]: 16,792-59,685) at the expense of 94,831 (95% UI: 84,827-105,630) overdiagnosed cancers. Age-based screening was the least cost-effective strategy studied. The greatest number of quality-adjusted life-years (QALYs) was generated by risk-based screening at a 10-year absolute risk threshold of 4%. At this threshold, risk-based screening led to one-third fewer overdiagnosed cancers (64,384, 95% UI: 57,382-72,050) but averted 6.3% fewer (9,695, 95% UI: 2,853-15,851) deaths from prostate cancer by comparison with age-based screening. Relative to no screening, risk-based screening at a 4% 10-year absolute risk threshold was cost-effective in 48.4% and 57.4% of the simulations at willingness-to-pay thresholds of GBP£20,000 (US$26,000) and £30,000 ($39,386) per QALY, respectively. The cost-effectiveness of risk-tailored screening improved as the threshold rose.
CONCLUSIONS
Based on the results of this modelling study, offering screening to men at higher risk could potentially reduce overdiagnosis and improve the benefit-harm tradeoff and the cost-effectiveness of a prostate cancer screening program. The optimal threshold will depend on societal judgements of the appropriate balance of benefits-harms and cost-effectiveness.
中文翻译:

前列腺癌的多基因风险定制筛查:一项效益-危害和成本效益模型研究。
背景美国预防服务工作组支持对 55-69 岁男性进行基于前列腺特异性抗原 (PSA) 筛查的个体化决策。了解筛查的潜在益处和危害如何随个人患前列腺癌的风险而变化,可以为个人和人群层面的筛查决策提供信息。该模型研究考察了与基于年龄的筛查和不进行筛查相比,针对风险定制的筛查计划的利弊权衡和成本效益。方法和结果 生命表模型是根据英格兰 448 万名 55 至 69 岁男性的假设队列开发的,该模型可预测特定年龄的前列腺癌发病率和死亡率,并随访至 90 岁。风险阈值基于年龄和多基因谱。我们比较了不筛查、基于年龄的筛查(从 55 岁到 69 岁的每四年一次 PSA 检测)和风险定制筛查(年龄在 55 岁到 69 岁之间,10 年绝对风险大于阈值的男性,从年龄开始接受四年一次的 PSA 检测)。达到风险阈值)。该分析是从卫生服务角度进行的,包括卫生系统承担风险评估、筛查、诊断和治疗的直接费用。我们使用概率敏感性分析来解释参数不确定性,并将未来成本和收益贴现为每年 3.5%。鉴于与我们的模型基于队列的结构相关的局限性以及数学模型中输入参数的不确定性,我们的分析应该谨慎考虑。 与 35 年随访期间未进行筛查相比,基于年龄的筛查预防了大多数前列腺癌死亡(39,272 例,95% 不确定区间 [UI]:16,792-59,685),但损失了 94,831 例(95% UI:84,827-105,630 例) )过度诊断的癌症。基于年龄的筛查是研究中成本效益最低的策略。最大数量的质量调整生命年 (QALY) 是通过基于风险的筛查产生的,10 年绝对风险阈值为 4%。在此阈值下,与相比,基于风险的筛查使过度诊断的癌症减少了三分之一(64,384,95% UI:57,382-72,050),但避免了前列腺癌死亡人数减少了 6.3%(9,695,95% UI:2,853-15,851)基于年龄的筛查。相对于不进行筛查,在 20,000 英镑(26,000 美元)和 30,000 英镑的支付意愿阈值下,4% 10 年绝对风险阈值的基于风险的筛查在 48.4% 和 57.4% 的模拟中具有成本效益每个 QALY 分别为 ($39,386)。随着门槛的提高,风险定制筛查的成本效益也随之提高。结论 根据这项模型研究的结果,为高风险男性提供筛查可能会减少过度诊断,并改善前列腺癌筛查计划的利弊权衡和成本效益。最佳阈值将取决于社会对利益-危害和成本效益之间适当平衡的判断。
更新日期:2020-01-14
中文翻译:
前列腺癌的多基因风险定制筛查:一项效益-危害和成本效益模型研究。
背景美国预防服务工作组支持对 55-69 岁男性进行基于前列腺特异性抗原 (PSA) 筛查的个体化决策。了解筛查的潜在益处和危害如何随个人患前列腺癌的风险而变化,可以为个人和人群层面的筛查决策提供信息。该模型研究考察了与基于年龄的筛查和不进行筛查相比,针对风险定制的筛查计划的利弊权衡和成本效益。方法和结果 生命表模型是根据英格兰 448 万名 55 至 69 岁男性的假设队列开发的,该模型可预测特定年龄的前列腺癌发病率和死亡率,并随访至 90 岁。风险阈值基于年龄和多基因谱。我们比较了不筛查、基于年龄的筛查(从 55 岁到 69 岁的每四年一次 PSA 检测)和风险定制筛查(年龄在 55 岁到 69 岁之间,10 年绝对风险大于阈值的男性,从年龄开始接受四年一次的 PSA 检测)。达到风险阈值)。该分析是从卫生服务角度进行的,包括卫生系统承担风险评估、筛查、诊断和治疗的直接费用。我们使用概率敏感性分析来解释参数不确定性,并将未来成本和收益贴现为每年 3.5%。鉴于与我们的模型基于队列的结构相关的局限性以及数学模型中输入参数的不确定性,我们的分析应该谨慎考虑。 与 35 年随访期间未进行筛查相比,基于年龄的筛查预防了大多数前列腺癌死亡(39,272 例,95% 不确定区间 [UI]:16,792-59,685),但损失了 94,831 例(95% UI:84,827-105,630 例) )过度诊断的癌症。基于年龄的筛查是研究中成本效益最低的策略。最大数量的质量调整生命年 (QALY) 是通过基于风险的筛查产生的,10 年绝对风险阈值为 4%。在此阈值下,与相比,基于风险的筛查使过度诊断的癌症减少了三分之一(64,384,95% UI:57,382-72,050),但避免了前列腺癌死亡人数减少了 6.3%(9,695,95% UI:2,853-15,851)基于年龄的筛查。相对于不进行筛查,在 20,000 英镑(26,000 美元)和 30,000 英镑的支付意愿阈值下,4% 10 年绝对风险阈值的基于风险的筛查在 48.4% 和 57.4% 的模拟中具有成本效益每个 QALY 分别为 ($39,386)。随着门槛的提高,风险定制筛查的成本效益也随之提高。结论 根据这项模型研究的结果,为高风险男性提供筛查可能会减少过度诊断,并改善前列腺癌筛查计划的利弊权衡和成本效益。最佳阈值将取决于社会对利益-危害和成本效益之间适当平衡的判断。










































 京公网安备 11010802027423号
京公网安备 11010802027423号