当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Long-Term Follow-Up of Complete Versus Lesion-Only Revascularization in STEMI and Multivessel Disease
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-12-01 , DOI: 10.1016/j.jacc.2019.10.033 Anthony H Gershlick 1 , Amerjeet S Banning 1 , Emma Parker 1 , Duolao Wang 2 , Charley A Budgeon 1 , Damian J Kelly 3 , Peter O Kane 4 , Miles Dalby 5 , Simon L Hetherington 6 , Gerry P McCann 1 , John P Greenwood 7 , Nick Curzen 8
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-12-01 , DOI: 10.1016/j.jacc.2019.10.033 Anthony H Gershlick 1 , Amerjeet S Banning 1 , Emma Parker 1 , Duolao Wang 2 , Charley A Budgeon 1 , Damian J Kelly 3 , Peter O Kane 4 , Miles Dalby 5 , Simon L Hetherington 6 , Gerry P McCann 1 , John P Greenwood 7 , Nick Curzen 8
Affiliation
|
BACKGROUND
Randomized trials have shown that complete revascularization in patients with ST-segment elevation myocardial infarction (MI) with multivessel disease results in lower major adverse cardiovascular events (MACE) (all-cause death, MI, ischemia-driven revascularization, heart failure). OBJECTIVES
The goal of this study was to determine whether the benefits of complete revascularization are sustained long-term and their impact on hard endpoints. METHODS
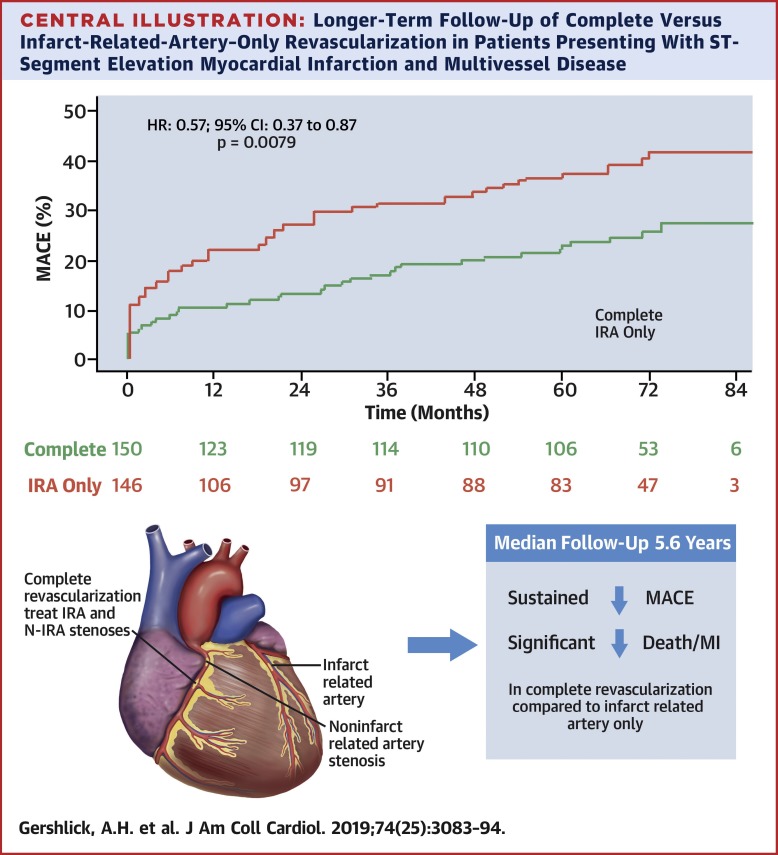
CvLPRIT (Complete versus Lesion-only Primary PCI Trial) was a randomized trial of complete inpatient revascularization versus infarct-related artery revascularization only at the index admission. Randomized patients have been followed longer-term. The components of the original primary endpoint were collected from physical and electronic patient records, and from local databases for all readmissions. RESULTS
The median follow-up (achieved in >90% patients) from randomization to first event or last follow-up was 5.6 years (0.0 to 7.3 years). The primary MACE endpoint rate at this time point was 24.0% in the complete revascularization group but 37.7% of the infarct-related artery-only group (hazard ratio: 0.57; 95% confidence interval: 0.37 to 0.87; p = 0.0079). The composite endpoint of all-cause death/MI was 10.0% in the complete revascularization group versus 18.5% in the infarct-related artery-only group (hazard ratio: 0.47; 95% confidence interval: 0.25 to 0.89; p = 0.0175). In a landmark analysis (from 12 months to final follow-up), there was no significant difference between MACE, death/MI, and individual components of the primary endpoint. CONCLUSIONS
Long-term follow-up of the CvLPRIT trial shows that the significantly lower rate of MACE in the complete revascularization group, previously seen at 12 months, is sustained to a median of 5.6 years. A significant difference in composite all-cause death/MI favoring the complete revascularization was also observed. (Complete versus Lesion-only Primary PCI Trial; ISRCTN70913605).
中文翻译:

STEMI 和多支血管疾病完全与仅病变血运重建的长期随访
背景随机试验表明,对患有多支血管疾病的 ST 段抬高型心肌梗死 (MI) 患者进行完全血运重建可降低主要不良心血管事件 (MACE)(全因死亡、MI、缺血驱动的血运重建、心力衰竭)。目的 本研究的目的是确定完全血运重建的益处是否能够长期持续及其对硬终点的影响。方法 CvLPRIT(完全与仅病变的主要 PCI 试验)是一项随机试验,仅在首次入院时进行完全住院血运重建与梗死相关动脉血运重建。对随机患者进行了长期随访。原始主要终点的组成部分是从物理和电子患者记录中收集的,以及所有重新入院的本地数据库。结果 从随机化到第一次事件或最后一次随访的中位随访时间(在 >90% 的患者中实现)为 5.6 年(0.0 至 7.3 年)。在这个时间点,完全血运重建组的主要 MACE 终点率为 24.0%,而仅梗死相关动脉组为 37.7%(风险比:0.57;95% 置信区间:0.37 至 0.87;p = 0.0079)。完全血运重建组的全因死亡 / MI 复合终点为 10.0%,而仅梗死相关动脉组为 18.5%(风险比:0.47;95% 置信区间:0.25 至 0.89;p = 0.0175)。在一项具有里程碑意义的分析(从 12 个月到最终随访)中,MACE、死亡/MI 和主要终点的各个组成部分之间没有显着差异。结论 CvLPRIT 试验的长期随访表明,完全血运重建组中显着较低的 MACE 发生率(先前在 12 个月时观察到)持续至中位数为 5.6 年。还观察到有利于完全血运重建的复合全因死亡/心肌梗死的显着差异。(完整与仅病变的主要 PCI 试验;ISRCTN70913605)。
更新日期:2019-12-01
中文翻译:
STEMI 和多支血管疾病完全与仅病变血运重建的长期随访
背景随机试验表明,对患有多支血管疾病的 ST 段抬高型心肌梗死 (MI) 患者进行完全血运重建可降低主要不良心血管事件 (MACE)(全因死亡、MI、缺血驱动的血运重建、心力衰竭)。目的 本研究的目的是确定完全血运重建的益处是否能够长期持续及其对硬终点的影响。方法 CvLPRIT(完全与仅病变的主要 PCI 试验)是一项随机试验,仅在首次入院时进行完全住院血运重建与梗死相关动脉血运重建。对随机患者进行了长期随访。原始主要终点的组成部分是从物理和电子患者记录中收集的,以及所有重新入院的本地数据库。结果 从随机化到第一次事件或最后一次随访的中位随访时间(在 >90% 的患者中实现)为 5.6 年(0.0 至 7.3 年)。在这个时间点,完全血运重建组的主要 MACE 终点率为 24.0%,而仅梗死相关动脉组为 37.7%(风险比:0.57;95% 置信区间:0.37 至 0.87;p = 0.0079)。完全血运重建组的全因死亡 / MI 复合终点为 10.0%,而仅梗死相关动脉组为 18.5%(风险比:0.47;95% 置信区间:0.25 至 0.89;p = 0.0175)。在一项具有里程碑意义的分析(从 12 个月到最终随访)中,MACE、死亡/MI 和主要终点的各个组成部分之间没有显着差异。结论 CvLPRIT 试验的长期随访表明,完全血运重建组中显着较低的 MACE 发生率(先前在 12 个月时观察到)持续至中位数为 5.6 年。还观察到有利于完全血运重建的复合全因死亡/心肌梗死的显着差异。(完整与仅病变的主要 PCI 试验;ISRCTN70913605)。










































 京公网安备 11010802027423号
京公网安备 11010802027423号