当前位置:
X-MOL 学术
›
JAMA Psychiatry
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Computational Markers of Risky Decision-making for Identification of Temporal Windows of Vulnerability to Opioid Use in a Real-world Clinical Setting.
JAMA Psychiatry ( IF 22.5 ) Pub Date : 2020-04-01 , DOI: 10.1001/jamapsychiatry.2019.4013 Anna B Konova 1, 2 , Silvia Lopez-Guzman 2, 3 , Adelya Urmanche 4 , Stephen Ross 4 , Kenway Louie 2, 5 , John Rotrosen 4 , Paul W Glimcher 2, 4
JAMA Psychiatry ( IF 22.5 ) Pub Date : 2020-04-01 , DOI: 10.1001/jamapsychiatry.2019.4013 Anna B Konova 1, 2 , Silvia Lopez-Guzman 2, 3 , Adelya Urmanche 4 , Stephen Ross 4 , Kenway Louie 2, 5 , John Rotrosen 4 , Paul W Glimcher 2, 4
Affiliation
|
Importance
Opioid addiction is a major public health problem. Despite availability of evidence-based treatments, relapse and dropout are common outcomes. Efforts aimed at identifying reuse risk and gaining more precise understanding of the mechanisms conferring reuse vulnerability are needed.
Objective
To use tools from computational psychiatry and decision neuroscience to identify changes in decision-making processes preceding opioid reuse.
Design, Setting, and Participants
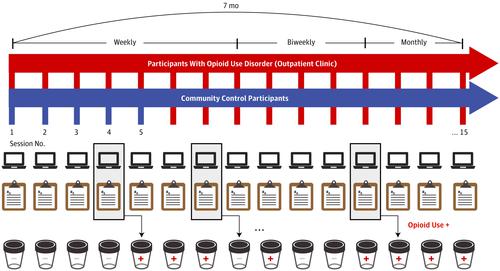
A cohort of individuals with opioid use disorder were studied longitudinally at a community-based treatment setting for up to 7 months (1-15 sessions per person). At each session, patients completed a risky decision-making task amenable to computational modeling and standard clinical assessments. Time-lagged mixed-effects logistic regression analyses were used to assess the likelihood of opioid use between sessions (t to t + 1; within the subsequent 1-4 weeks) from data acquired at the current session (t). A cohort of control participants completed similar procedures (1-5 sessions per person), serving both as a baseline comparison group and an independent sample in which to assess measurement test-retest reliability. Data were analyzed between January 1, 2018, and September 5, 2019.
Main Outcomes and Measures
Two individual model-based behavioral markers were derived from the task completed at each session, capturing a participant's current tolerance of known risks and ambiguity (partially unknown risks). Current anxiety, craving, withdrawal, and nonadherence were assessed via interview and clinic records. Opioid use was ascertained from random urine toxicology tests and self-reports.
Results
Seventy patients (mean [SE] age, 44.7 [1.3] years; 12 women and 58 men [82.9% male]) and 55 control participants (mean [SE] age, 42.4 [1.5] years; 13 women and 42 men [76.4% male]) were included. Of the 552 sessions completed with patients (mean [SE], 7.89 [0.59] sessions per person), 252 (45.7%) directly preceded opioid use events (mean [SE], 3.60 [0.44] sessions per person). From the task parameters, only ambiguity tolerance was significantly associated with increased odds of prospective opioid use (adjusted odds ratio, 1.37 [95% CI, 1.07-1.76]), indicating patients were more tolerant specifically of ambiguous risks prior to these use events. The association of ambiguity tolerance with prospective use was independent of established clinical factors (adjusted odds ratio, 1.29 [95% CI, 1.01-1.65]; P = .04), such that a model combining these factors explained more variance in reuse risk. No significant differences in ambiguity tolerance were observed between patients and control participants, who completed 197 sessions (mean [SE], 3.58 [0.21] sessions per person); however, patients were more tolerant of known risks (B = 0.56 [95% CI, 0.05-1.07]).
Conclusions and Relevance
Computational approaches can provide mechanistic insights about the cognitive factors underlying opioid reuse vulnerability and may hold promise for clinical use.
中文翻译:

风险决策的计算标记,用于确定在实际临床环境中对使用阿片类药物的脆弱性的时间窗。
重要性阿片类药物成瘾是主要的公共卫生问题。尽管可以使用循证疗法,但复发和辍学是常见的结局。需要做出努力以识别重用风险并更准确地了解造成重用漏洞的机制。目的使用来自计算精神病学和决策神经科学的工具来识别阿片类药物再利用之前决策过程中的变化。设计,环境和参与者在基于社区的治疗环境中,对一组阿片类药物使用障碍患者进行了纵向研究,长达7个月(每人1至15次治疗)。在每次会议中,患者都要完成适合计算模型和标准临床评估的危险决策任务。使用时滞混合效应逻辑回归分析,从当前疗程(t)获得的数据评估各疗程之间使用阿片类药物的可能性(t至t + 1;在随后的1-4周内)。一组对照参与者完成了类似的程序(每人1-5次),既作为基线比较组,又作为独立样本来评估测量重测信度。分析了2018年1月1日至2019年9月5日之间的数据。主要结果和措施从每次会议完成的任务中得出两个基于模型的行为标记,捕获参与者当前对已知风险和歧义(部分未知风险)的容忍度)。通过访谈和临床记录评估当前的焦虑,渴望,戒断和不依从情况。阿片类药物的使用是通过随机尿毒理学测试和自我报告确定的。结果70名患者(平均[SE]年龄,44.7 [1.3]岁; 12名女性和58名男性[82.9%男性])和55名对照参与者(平均[SE]年龄,42.4 [1.5]岁; 13名女性和42名男性[男性占76.4%)。在患者共完成的552次疗程中(平均[SE],每人7.89 [0.59]次疗程),其中有252次(45.7%)直接在阿片类药物使用事件之前(平均[SE],每人3.60 [0.44]次疗程)。从任务参数来看,仅歧义耐受性与预期使用阿片类药物的几率显着相关(调整后的几率比为1.37 [95%CI,1.07-1.76]),表明患者在这些使用事件发生之前对歧义性风险的耐受性更高。歧义耐受性与前瞻性使用之间的关联与既定的临床因素无关(调整后的优势比为1.29 [95%CI,1.01-1.65]; P = .04),因此结合这些因素的模型解释了重复使用风险的更多差异。患者和对照组参与者完成197节(平均[SE],每人3.58 [0.21]节)时,在歧义容忍度上没有观察到显着差异。但是,患者对已知风险的耐受性更高(B = 0.56 [95%CI,0.05-1.07])。结论与相关性计算方法可以提供有关阿片类药物再利用易损性的认知因素的机械见解,并可能为临床使用带来希望。患者和对照组参与者完成197节(平均[SE],每人3.58 [0.21]节)时,在歧义容忍度上没有观察到显着差异。但是,患者对已知风险的耐受性更高(B = 0.56 [95%CI,0.05-1.07])。结论与相关性计算方法可以提供有关阿片类药物再利用易损性的认知因素的机械见解,并可能为临床使用带来希望。患者和对照组参与者完成197节(平均[SE],每人3.58 [0.21]节)时,在歧义容忍度上没有观察到显着差异。但是,患者对已知风险的耐受性更高(B = 0.56 [95%CI,0.05-1.07])。结论与相关性计算方法可以提供有关阿片类药物再利用易损性的认知因素的机械见解,并可能为临床使用带来希望。
更新日期:2020-04-01
中文翻译:
风险决策的计算标记,用于确定在实际临床环境中对使用阿片类药物的脆弱性的时间窗。
重要性阿片类药物成瘾是主要的公共卫生问题。尽管可以使用循证疗法,但复发和辍学是常见的结局。需要做出努力以识别重用风险并更准确地了解造成重用漏洞的机制。目的使用来自计算精神病学和决策神经科学的工具来识别阿片类药物再利用之前决策过程中的变化。设计,环境和参与者在基于社区的治疗环境中,对一组阿片类药物使用障碍患者进行了纵向研究,长达7个月(每人1至15次治疗)。在每次会议中,患者都要完成适合计算模型和标准临床评估的危险决策任务。使用时滞混合效应逻辑回归分析,从当前疗程(t)获得的数据评估各疗程之间使用阿片类药物的可能性(t至t + 1;在随后的1-4周内)。一组对照参与者完成了类似的程序(每人1-5次),既作为基线比较组,又作为独立样本来评估测量重测信度。分析了2018年1月1日至2019年9月5日之间的数据。主要结果和措施从每次会议完成的任务中得出两个基于模型的行为标记,捕获参与者当前对已知风险和歧义(部分未知风险)的容忍度)。通过访谈和临床记录评估当前的焦虑,渴望,戒断和不依从情况。阿片类药物的使用是通过随机尿毒理学测试和自我报告确定的。结果70名患者(平均[SE]年龄,44.7 [1.3]岁; 12名女性和58名男性[82.9%男性])和55名对照参与者(平均[SE]年龄,42.4 [1.5]岁; 13名女性和42名男性[男性占76.4%)。在患者共完成的552次疗程中(平均[SE],每人7.89 [0.59]次疗程),其中有252次(45.7%)直接在阿片类药物使用事件之前(平均[SE],每人3.60 [0.44]次疗程)。从任务参数来看,仅歧义耐受性与预期使用阿片类药物的几率显着相关(调整后的几率比为1.37 [95%CI,1.07-1.76]),表明患者在这些使用事件发生之前对歧义性风险的耐受性更高。歧义耐受性与前瞻性使用之间的关联与既定的临床因素无关(调整后的优势比为1.29 [95%CI,1.01-1.65]; P = .04),因此结合这些因素的模型解释了重复使用风险的更多差异。患者和对照组参与者完成197节(平均[SE],每人3.58 [0.21]节)时,在歧义容忍度上没有观察到显着差异。但是,患者对已知风险的耐受性更高(B = 0.56 [95%CI,0.05-1.07])。结论与相关性计算方法可以提供有关阿片类药物再利用易损性的认知因素的机械见解,并可能为临床使用带来希望。患者和对照组参与者完成197节(平均[SE],每人3.58 [0.21]节)时,在歧义容忍度上没有观察到显着差异。但是,患者对已知风险的耐受性更高(B = 0.56 [95%CI,0.05-1.07])。结论与相关性计算方法可以提供有关阿片类药物再利用易损性的认知因素的机械见解,并可能为临床使用带来希望。患者和对照组参与者完成197节(平均[SE],每人3.58 [0.21]节)时,在歧义容忍度上没有观察到显着差异。但是,患者对已知风险的耐受性更高(B = 0.56 [95%CI,0.05-1.07])。结论与相关性计算方法可以提供有关阿片类药物再利用易损性的认知因素的机械见解,并可能为临床使用带来希望。









































 京公网安备 11010802027423号
京公网安备 11010802027423号