当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Impact of Renal Impairment on Beta-Blocker Efficacy in Patients With Heart Failure
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-12-01 , DOI: 10.1016/j.jacc.2019.09.059 Dipak Kotecha 1 , Simrat K Gill 2 , Marcus D Flather 3 , Jane Holmes 4 , Milton Packer 5 , Giuseppe Rosano 6 , Michael Böhm 7 , John J V McMurray 8 , John Wikstrand 9 , Stefan D Anker 10 , Dirk J van Veldhuisen 11 , Luis Manzano 12 , Thomas G von Lueder 13 , Alan S Rigby 14 , Bert Andersson 15 , John Kjekshus 16 , Hans Wedel 17 , Frank Ruschitzka 18 , John G F Cleland 19 , Kevin Damman 11 , Josep Redon 20 , Andrew J S Coats 6 ,
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-12-01 , DOI: 10.1016/j.jacc.2019.09.059 Dipak Kotecha 1 , Simrat K Gill 2 , Marcus D Flather 3 , Jane Holmes 4 , Milton Packer 5 , Giuseppe Rosano 6 , Michael Böhm 7 , John J V McMurray 8 , John Wikstrand 9 , Stefan D Anker 10 , Dirk J van Veldhuisen 11 , Luis Manzano 12 , Thomas G von Lueder 13 , Alan S Rigby 14 , Bert Andersson 15 , John Kjekshus 16 , Hans Wedel 17 , Frank Ruschitzka 18 , John G F Cleland 19 , Kevin Damman 11 , Josep Redon 20 , Andrew J S Coats 6 ,
Affiliation
|
BACKGROUND
Moderate and moderately severe renal impairment are common in patients with heart failure and reduced ejection fraction, but whether beta-blockers are effective is unclear, leading to underuse of life-saving therapy. OBJECTIVES
This study sought to investigate patient prognosis and the efficacy of beta-blockers according to renal function using estimated glomerular filtration rate (eGFR). METHODS
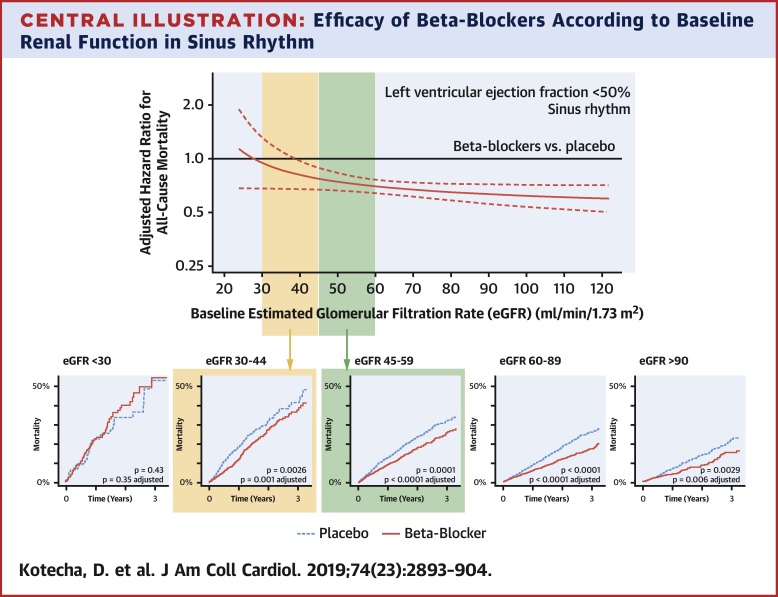
Analysis of 16,740 individual patients with left ventricular ejection fraction <50% from 10 double-blind, placebo-controlled trials was performed. The authors report all-cause mortality on an intention-to-treat basis, adjusted for baseline covariates and stratified by heart rhythm. RESULTS
Median eGFR at baseline was 63 (interquartile range: 50 to 77) ml/min/1.73 m2; 4,584 patients (27.4%) had eGFR 45 to 59 ml/min/1.73 m2, and 2,286 (13.7%) 30 to 44 ml/min/1.73 m2. Over a median follow-up of 1.3 years, eGFR was independently associated with mortality, with a 12% higher risk of death for every 10 ml/min/1.73 m2 lower eGFR (95% confidence interval [CI]: 10% to 15%; p < 0.001). In 13,861 patients in sinus rhythm, beta-blockers reduced mortality versus placebo; adjusted hazard ratio (HR): 0.73 for eGFR 45 to 59 ml/min/1.73 m2 (95% CI: 0.62 to 0.86; p < 0.001) and 0.71 for eGFR 30 to 44 ml/min/1.73 m2 (95% CI: 0.58 to 0.87; p = 0.001). The authors observed no deterioration in renal function over time in patients with moderate or moderately severe renal impairment, no difference in adverse events comparing beta-blockers with placebo, and higher mortality in patients with worsening renal function on follow-up. Due to exclusion criteria, there were insufficient patients with severe renal dysfunction (eGFR <30 ml/min/1.73 m2) to draw conclusions. In 2,879 patients with atrial fibrillation, there was no reduction in mortality with beta-blockers at any level of eGFR. CONCLUSIONS
Patients with heart failure, left ventricular ejection fraction <50% and sinus rhythm should receive beta-blocker therapy even with moderate or moderately severe renal dysfunction.
中文翻译:

肾损伤对心力衰竭患者 β 受体阻滞剂疗效的影响
背景 中度和中度重度肾功能损害在心力衰竭和射血分数降低的患者中很常见,但β受体阻滞剂是否有效尚不清楚,导致救生治疗的使用不足。目的 本研究旨在使用估计肾小球滤过率(eGFR)根据肾功能研究患者预后和 β 受体阻滞剂的疗效。方法 对 10 项双盲、安慰剂对照试验中的 16,740 名左心室射血分数 <50% 的患者进行分析。作者报告了意向治疗基础上的全因死亡率,根据基线协变量进行调整并按心律进行分层。结果 基线时 eGFR 中位数为 63(四分位数范围:50 至 77)ml/min/1.73 m2; 4,584 名患者 (27.4%) 的 eGFR 为 45 至 59 ml/min/1.73 m2,2,286 名患者 (13.7%) 的 eGFR 为 30 至 44 ml/min/1.73 m2。在中位随访 1.3 年中,eGFR 与死亡率独立相关,eGFR 每降低 10 ml/min/1.73 m2,死亡风险就会增加 12%(95% 置信区间 [CI]:10% 至 15%) ;p<0.001)。在 13,861 名窦性心律患者中,β-受体阻滞剂与安慰剂相比降低了死亡率;调整后的风险比 (HR):eGFR 45 至 59 ml/min/1.73 m2 为 0.73(95% CI:0.62 至 0.86;p < 0.001),eGFR 30 至 44 ml/min/1.73 m2 为 0.71(95% CI: 0.58 至 0.87;p = 0.001)。作者观察到,随着时间的推移,中度或中度重度肾功能不全患者的肾功能没有恶化,β-受体阻滞剂与安慰剂相比,不良事件没有差异,并且随访时肾功能恶化的患者死亡率更高。由于排除标准,没有足够的严重肾功能不全(eGFR <30 ml/min/1.73 m2)患者得出结论。 在 2,879 名房颤患者中,β 受体阻滞剂在任何 eGFR 水平下均未降低死亡率。结论心力衰竭、左心室射血分数<50%和窦性心律的患者即使患有中度或中度重度肾功能不全也应接受β受体阻滞剂治疗。
更新日期:2019-12-01
中文翻译:
肾损伤对心力衰竭患者 β 受体阻滞剂疗效的影响
背景 中度和中度重度肾功能损害在心力衰竭和射血分数降低的患者中很常见,但β受体阻滞剂是否有效尚不清楚,导致救生治疗的使用不足。目的 本研究旨在使用估计肾小球滤过率(eGFR)根据肾功能研究患者预后和 β 受体阻滞剂的疗效。方法 对 10 项双盲、安慰剂对照试验中的 16,740 名左心室射血分数 <50% 的患者进行分析。作者报告了意向治疗基础上的全因死亡率,根据基线协变量进行调整并按心律进行分层。结果 基线时 eGFR 中位数为 63(四分位数范围:50 至 77)ml/min/1.73 m2; 4,584 名患者 (27.4%) 的 eGFR 为 45 至 59 ml/min/1.73 m2,2,286 名患者 (13.7%) 的 eGFR 为 30 至 44 ml/min/1.73 m2。在中位随访 1.3 年中,eGFR 与死亡率独立相关,eGFR 每降低 10 ml/min/1.73 m2,死亡风险就会增加 12%(95% 置信区间 [CI]:10% 至 15%) ;p<0.001)。在 13,861 名窦性心律患者中,β-受体阻滞剂与安慰剂相比降低了死亡率;调整后的风险比 (HR):eGFR 45 至 59 ml/min/1.73 m2 为 0.73(95% CI:0.62 至 0.86;p < 0.001),eGFR 30 至 44 ml/min/1.73 m2 为 0.71(95% CI: 0.58 至 0.87;p = 0.001)。作者观察到,随着时间的推移,中度或中度重度肾功能不全患者的肾功能没有恶化,β-受体阻滞剂与安慰剂相比,不良事件没有差异,并且随访时肾功能恶化的患者死亡率更高。由于排除标准,没有足够的严重肾功能不全(eGFR <30 ml/min/1.73 m2)患者得出结论。 在 2,879 名房颤患者中,β 受体阻滞剂在任何 eGFR 水平下均未降低死亡率。结论心力衰竭、左心室射血分数<50%和窦性心律的患者即使患有中度或中度重度肾功能不全也应接受β受体阻滞剂治疗。










































 京公网安备 11010802027423号
京公网安备 11010802027423号