当前位置:
X-MOL 学术
›
Modern Pathol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Melanoma pathology reporting and staging.
Modern Pathology ( IF 7.1 ) Pub Date : 2019-11-22 , DOI: 10.1038/s41379-019-0402-x Richard A Scolyer 1, 2, 3 , Robert V Rawson 1, 2, 3 , Jeffrey E Gershenwald 4 , Peter M Ferguson 1, 2, 3 , Victor G Prieto 4
Modern Pathology ( IF 7.1 ) Pub Date : 2019-11-22 , DOI: 10.1038/s41379-019-0402-x Richard A Scolyer 1, 2, 3 , Robert V Rawson 1, 2, 3 , Jeffrey E Gershenwald 4 , Peter M Ferguson 1, 2, 3 , Victor G Prieto 4
Affiliation
|
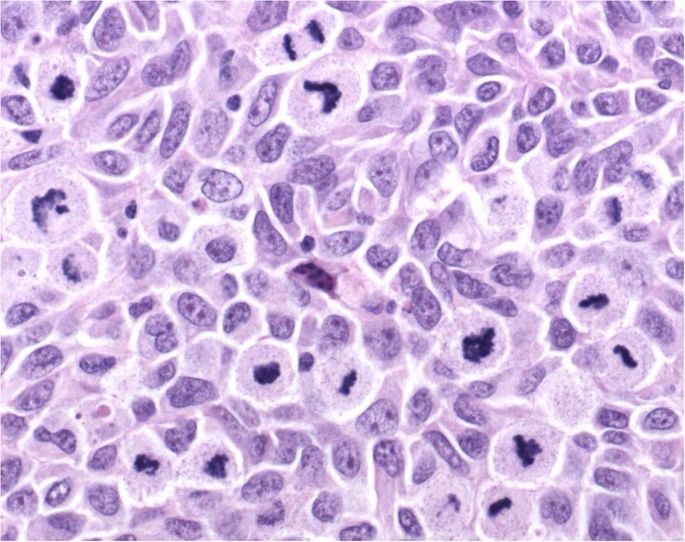
The pathological diagnosis of melanoma can be challenging. The provision of an appropriate biopsy and pertinent history can assist in establishing an accurate diagnosis and reliable estimate of prognosis. In their reports, pathologists should document both the criteria on which the diagnosis was based as well as important prognostic parameters. For melanoma, such prognostic parameters include tumor thickness, ulceration, mitotic rate, lymphovascular invasion, neurotropism, and tumor-infiltrating lymphocytes. Disease staging is important for risk stratifying melanoma patients into prognostic groups and patient management recommendations are often stage based. The 8th edition American Joint Committee on Cancer (AJCC) Melanoma Staging System was implemented in 2018 and several important changes were made. Tumor thickness and ulceration remain the key T category criteria. T1b melanomas were redefined as either ulcerated melanomas <1.0 mm thick or nonulcerated melanomas 0.8-1.0 mm thick. Although mitotic rate was removed as a T category criterion in the 8th edition, it remains a very important prognostic factor and should continue to be documented in primary melanoma pathology reports. It was also recommended in the 8th edition that tumor thickness be recorded to the nearest 0.1 mm (rather than the nearest 0.01 mm). In the future, incorporation of additional prognostic parameters beyond those utilized in the current version of the staging system into (web based) prognostic models/clinical tools will likely facilitate more personalized prognostic estimates. Evaluation of molecular markers of prognosis is an active area of current research; however, additional data are needed before it would be appropriate to recommend use of such tests in routine clinical practice.
中文翻译:

黑色素瘤病理学报告和分期。
黑色素瘤的病理诊断可能具有挑战性。提供适当的活检和相关病史有助于建立准确的诊断和可靠的预后估计。在他们的报告中,病理学家应记录诊断所依据的标准以及重要的预后参数。对于黑色素瘤,此类预后参数包括肿瘤厚度、溃疡、有丝分裂率、淋巴血管浸润、神经趋向性和肿瘤浸润淋巴细胞。疾病分期对于将黑色素瘤患者风险分层为预后组很重要,患者管理建议通常基于分期。第 8 版美国癌症联合委员会 (AJCC) 黑色素瘤分期系统于 2018 年实施,并进行了几项重要更改。肿瘤厚度和溃疡仍然是关键的 T 分类标准。T1b 黑色素瘤被重新定义为厚度小于 1.0 毫米的溃疡性黑色素瘤或厚度为 0.8-1.0 毫米的非溃疡性黑色素瘤。尽管在第 8 版中不再将有丝分裂率作为 T 分类标准,但它仍然是一个非常重要的预后因素,应继续记录在原发性黑色素瘤病理学报告中。第 8 版还建议将肿瘤厚度记录到最接近的 0.1 毫米(而不是最接近的 0.01 毫米)。将来,将当前版本的分期系统中使用的参数以外的其他预后参数纳入(基于网络的)预后模型/临床工具可能会促进更个性化的预后估计。预后分子标志物的评估是当前研究的一个活跃领域;然而,
更新日期:2019-11-22
中文翻译:
黑色素瘤病理学报告和分期。
黑色素瘤的病理诊断可能具有挑战性。提供适当的活检和相关病史有助于建立准确的诊断和可靠的预后估计。在他们的报告中,病理学家应记录诊断所依据的标准以及重要的预后参数。对于黑色素瘤,此类预后参数包括肿瘤厚度、溃疡、有丝分裂率、淋巴血管浸润、神经趋向性和肿瘤浸润淋巴细胞。疾病分期对于将黑色素瘤患者风险分层为预后组很重要,患者管理建议通常基于分期。第 8 版美国癌症联合委员会 (AJCC) 黑色素瘤分期系统于 2018 年实施,并进行了几项重要更改。肿瘤厚度和溃疡仍然是关键的 T 分类标准。T1b 黑色素瘤被重新定义为厚度小于 1.0 毫米的溃疡性黑色素瘤或厚度为 0.8-1.0 毫米的非溃疡性黑色素瘤。尽管在第 8 版中不再将有丝分裂率作为 T 分类标准,但它仍然是一个非常重要的预后因素,应继续记录在原发性黑色素瘤病理学报告中。第 8 版还建议将肿瘤厚度记录到最接近的 0.1 毫米(而不是最接近的 0.01 毫米)。将来,将当前版本的分期系统中使用的参数以外的其他预后参数纳入(基于网络的)预后模型/临床工具可能会促进更个性化的预后估计。预后分子标志物的评估是当前研究的一个活跃领域;然而,








































 京公网安备 11010802027423号
京公网安备 11010802027423号