Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Substance use disorders in refugee and migrant groups in Sweden: A nationwide cohort study of 1.2 million people.
PLOS Medicine ( IF 10.5 ) Pub Date : 2019-11-05 , DOI: 10.1371/journal.pmed.1002944 Samantha Harris 1, 2 , Jennifer Dykxhoorn 1 , Anna-Clara Hollander 3 , Christina Dalman 3 , James B Kirkbride 1
PLOS Medicine ( IF 10.5 ) Pub Date : 2019-11-05 , DOI: 10.1371/journal.pmed.1002944 Samantha Harris 1, 2 , Jennifer Dykxhoorn 1 , Anna-Clara Hollander 3 , Christina Dalman 3 , James B Kirkbride 1
Affiliation
|
BACKGROUND
Refugees are at higher risk of some psychiatric disorders, including post-traumatic stress disorder (PTSD) and psychosis, compared with other non-refugee migrants and the majority population. However, it is unclear whether this also applies to substance use disorders, which we investigated in a national register cohort study in Sweden. We also investigated whether risk varied by region of origin, age at migration, time in Sweden, and diagnosis of PTSD.
METHODS AND FINDINGS
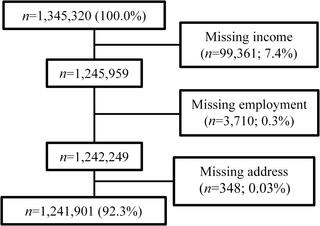
Using linked Swedish register data, we followed a cohort born between 1984 and 1997 from their 14th birthday or arrival in Sweden, if later, until an International Classification of Diseases, 10th revision (ICD-10), diagnosis of substance use disorder (codes F10.X-19.X), emigration, death, or end of follow-up (31 December 2016). Refugee and non-refugee migrants were restricted to those from regions with at least 1,000 refugees in the Swedish registers. We used Cox proportional hazards regression to estimate unadjusted and adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) in refugee and non-refugee migrants, compared with Swedish-born individuals, for all substance use disorders (F10.X-19.X), alcohol use disorders (F10.X), cannabis use disorders (F12.X), and polydrug use disorders (F19.X). In adjusted analyses, we controlled for age, sex, birth year, family income, family employment status, population density, and PTSD diagnosis. Our sample of 1,241,901 participants included 17,783 (1.4%) refugee and 104,250 (8.4%) non-refugee migrants. Refugees' regions of origin were represented in proportions ranging from 6.0% (Eastern Europe and Russia) to 41.4% (Middle East and North Africa); proportions of non-refugee migrants' regions of origin ranged from 11.8% (sub-Saharan Africa) to 33.7% (Middle East and North Africa). These groups were more economically disadvantaged at cohort entry (p < 0.001) than the Swedish-born population. Refugee (aHR: 0.52; 95% CI 0.46-0.60) and non-refugee (aHR: 0.46; 95% CI 0.43-0.49) migrants had similarly lower rates of all substance use disorders compared with Swedish-born individuals (crude incidence: 290.2 cases per 100,000 person-years; 95% CI 287.3-293.1). Rates of substance use disorders in migrants converged to the Swedish-born rate over time, indicated by both earlier age at migration and longer time in Sweden. We observed similar patterns for alcohol and polydrug use disorders, separately, although differences in cannabis use were less marked; findings did not differ substantially by migrants' region of origin. Finally, while a PTSD diagnosis was over 5 times more common in refugees than the Swedish-born population, it was more strongly associated with increased rates of substance use disorders in the Swedish-born population (aHR: 7.36; 95% CI 6.79-7.96) than non-refugee migrants (HR: 4.88; 95% CI 3.71-6.41; likelihood ratio test [LRT]: p = 0.01). The main limitations of our study were possible non-differential or differential under-ascertainment (by migrant status) of those only seen via primary care and that our findings may not generalize to undocumented migrants, who were not part of this study.
CONCLUSIONS
Our findings suggest that lower rates of substance use disorders in migrants and refugees may reflect prevalent behaviors with respect to substance use in migrants' countries of origin, although this effect appeared to diminish over time in Sweden, with rates converging towards the substantial burden of substance use morbidity we observed in the Swedish-born population.
中文翻译:

瑞典难民和移民群体中的物质使用障碍:一项针对120万人的全国性队列研究。
背景技术与其他非难民移民和多数人口相比,难民处于某些精神疾病的较高风险中,包括创伤后应激障碍(PTSD)和精神病。但是,尚不清楚这是否也适用于物质使用障碍,我们在瑞典的一项国家注册队列研究中对此进行了调查。我们还调查了风险是否因来源地区,迁徙年龄,瑞典时间和PTSD诊断而异。方法和调查结果:我们使用瑞典的相关登记数据,追踪了从1984年至1997年出生的14岁生日或到达瑞典的队列。 (代码F10.X-19.X),移民,死亡或后续行动结束(2016年12月31日)。难民和非难民移民仅限于瑞典籍册中至少有1,000名难民的地区的移民。与瑞典出生的个体相比,我们使用Cox比例风险回归来估计所有物质使用失调的难民和非难民移民的未经调整和调整后的风险比(aHRs)和95%置信区间(CIs)(F10.X-19 .X),酒精使用障碍(F10.X),大麻使用障碍(F12.X)和多药使用障碍(F19.X)。在调整后的分析中,我们控制了年龄,性别,出生年份,家庭收入,家庭就业状况,人口密度和PTSD诊断。我们的1,241,901名参与者样本包括17,783(1.4%)难民和104,250(8.4%)非难民移民。难民的原籍地区所占比例为6.0%(东欧和俄罗斯)至41%。4%(中东和北非);非难民移民的原籍地区比例从11.8%(撒哈拉以南非洲)到33.7%(中东和北非)不等。与瑞典出生的人群相比,这些人群在进入队列时在经济上处于不利地位(p <0.001)。与瑞典出生的个体相比,难民(aHR:0.52; 95%CI 0.46-0.60)和非难民(aHR:0.46; 95%CI 0.43-0.49)移民的所有物质使用失调的发生率均低于瑞典出生的个体(粗发病率:290.2)每100,000人年(95%CI 287.3-293.1)。随着时间的推移,移徙者的年龄增长和瑞典较长的时间都表明,移徙者中的物质使用失调的比率随着时间的推移逐渐收敛到瑞典出生的比率。我们分别观察到酒精和多种药物使用障碍的相似模式,尽管大麻使用的差异不太明显。调查结果在移民的原籍地上并没有很大的不同。最后,虽然创伤后创伤后应激障碍的诊断在难民中的发生率是瑞典出生人口的5倍以上,但与瑞典出生人口中药物滥用失调的发生率相关性更高(aHR:7.36; 95%CI 6.79-7.96) )比非难民移民(HR:4.88; 95%CI 3.71-6.41;似然比检验[LRT]:p = 0.01)。我们研究的主要局限性是对那些仅通过初级保健就诊的患者可能进行的非鉴别性或鉴别性不足(按移民身份),并且我们的发现可能不会推广到没有证件的移民,他们不是本研究的一部分。结论我们的研究结果表明,移民和难民中较低的吸毒成瘾率可能反映出移民中滥用毒品的普遍行为
更新日期:2019-12-03
中文翻译:
瑞典难民和移民群体中的物质使用障碍:一项针对120万人的全国性队列研究。
背景技术与其他非难民移民和多数人口相比,难民处于某些精神疾病的较高风险中,包括创伤后应激障碍(PTSD)和精神病。但是,尚不清楚这是否也适用于物质使用障碍,我们在瑞典的一项国家注册队列研究中对此进行了调查。我们还调查了风险是否因来源地区,迁徙年龄,瑞典时间和PTSD诊断而异。方法和调查结果:我们使用瑞典的相关登记数据,追踪了从1984年至1997年出生的14岁生日或到达瑞典的队列。 (代码F10.X-19.X),移民,死亡或后续行动结束(2016年12月31日)。难民和非难民移民仅限于瑞典籍册中至少有1,000名难民的地区的移民。与瑞典出生的个体相比,我们使用Cox比例风险回归来估计所有物质使用失调的难民和非难民移民的未经调整和调整后的风险比(aHRs)和95%置信区间(CIs)(F10.X-19 .X),酒精使用障碍(F10.X),大麻使用障碍(F12.X)和多药使用障碍(F19.X)。在调整后的分析中,我们控制了年龄,性别,出生年份,家庭收入,家庭就业状况,人口密度和PTSD诊断。我们的1,241,901名参与者样本包括17,783(1.4%)难民和104,250(8.4%)非难民移民。难民的原籍地区所占比例为6.0%(东欧和俄罗斯)至41%。4%(中东和北非);非难民移民的原籍地区比例从11.8%(撒哈拉以南非洲)到33.7%(中东和北非)不等。与瑞典出生的人群相比,这些人群在进入队列时在经济上处于不利地位(p <0.001)。与瑞典出生的个体相比,难民(aHR:0.52; 95%CI 0.46-0.60)和非难民(aHR:0.46; 95%CI 0.43-0.49)移民的所有物质使用失调的发生率均低于瑞典出生的个体(粗发病率:290.2)每100,000人年(95%CI 287.3-293.1)。随着时间的推移,移徙者的年龄增长和瑞典较长的时间都表明,移徙者中的物质使用失调的比率随着时间的推移逐渐收敛到瑞典出生的比率。我们分别观察到酒精和多种药物使用障碍的相似模式,尽管大麻使用的差异不太明显。调查结果在移民的原籍地上并没有很大的不同。最后,虽然创伤后创伤后应激障碍的诊断在难民中的发生率是瑞典出生人口的5倍以上,但与瑞典出生人口中药物滥用失调的发生率相关性更高(aHR:7.36; 95%CI 6.79-7.96) )比非难民移民(HR:4.88; 95%CI 3.71-6.41;似然比检验[LRT]:p = 0.01)。我们研究的主要局限性是对那些仅通过初级保健就诊的患者可能进行的非鉴别性或鉴别性不足(按移民身份),并且我们的发现可能不会推广到没有证件的移民,他们不是本研究的一部分。结论我们的研究结果表明,移民和难民中较低的吸毒成瘾率可能反映出移民中滥用毒品的普遍行为










































 京公网安备 11010802027423号
京公网安备 11010802027423号