JACC: Heart Failure ( IF 10.3 ) Pub Date : 2019-10-09 , DOI: 10.1016/j.jchf.2019.07.010 Joost C Beusekamp 1 , Jasper Tromp 2 , John G F Cleland 3 , Michael M Givertz 4 , Marco Metra 5 , Christopher M O'Connor 6 , John R Teerlink 7 , Piotr Ponikowski 8 , Wouter Ouwerkerk 9 , Dirk J van Veldhuisen 1 , Adriaan A Voors 1 , Peter van der Meer 1
|
Objectives
This study investigated associations between incident hyperkalemia during acute heart failure (HF) hospitalizations and changes in renin-angiotensin-aldosterone system (RAAS) inhibitors.
Background
Hyperkalemia is a potential complication of RAAS inhibitors. For patients with HF, fear of hyperkalemia may lead to failure to deliver guideline-recommended doses of RAAS inhibitors.
Methods
Serum potassium concentrations were measured daily from baseline (<24 h after admission) until discharge or day 7 in 1,589 patients enrolled in the PROTECT (Placebo-Controlled Randomized Study of the Selective A1 Adenosine Receptor Antagonist Rolofylline for Patients Hospitalized with Acute Decompensated Heart Failure and Volume Overload to Assess Treatment Effect on Congestion and Renal Function) trial. Incident hyperkalemia was defined as at least 1 episode of potassium >5.0 mEq/l. The primary outcome was all-cause mortality at 180 days.
Results
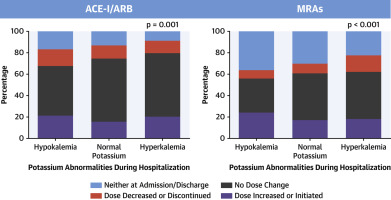
Overall, serum potassium concentrations increased from 4.3 ± 0.6 mEq/l at baseline to 4.5 ± 0.6 mEq/l at discharge or day 7 (p < 0.001). Patients developing incident hyperkalemia (n = 564; 35%) were more often taking mineralocorticoid antagonists (MRAs) therapy prior to hospitalization and were more likely to have them down-titrated during hospitalization, independent of confounders. Incident hyperkalemia was not associated with adverse outcomes. Yet, down-titration of MRAs during hospitalization was independently associated with 180-day mortality (hazard ratio [HR]: 1.73; 95% confidence interval [CI]: 1.15 to 2.60), regardless of incident hyperkalemia (pinteraction >0.10). Patients with incident hyperkalemia who were discharged with the same or increased dose of MRAs (HR: 0.52; 95% CI: 0.32 to 0.85) or angiotensin-converting enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs) (HR: 0.47; 95% CI: 0.29 to 0.77) had a lower 180-day mortality.
Conclusions
Incident hyperkalemia is common in patients hospitalized for acute HF and is not associated with adverse outcomes. Incident hyperkalemia is associated with down-titration of MRAs, but patients who maintained or increased their dose of MRAs and/or ACE inhibitors/ARB during acute HF hospitalization had better 180-day survival.
中文翻译:
急性心力衰竭住院期间的高钾血症和RAAS抑制剂治疗及其与死亡率的关系。
目标
这项研究调查了急性心力衰竭(HF)住院期间发生的高钾血症与肾素-血管紧张素-醛固酮系统(RAAS)抑制剂变化之间的关联。
背景
高钾血症是RAAS抑制剂的潜在并发症。对于心力衰竭患者,对高钾血症的恐惧可能导致无法提供指南推荐剂量的RAAS抑制剂。
方法
每天从基线(入院后24小时)直至出院或第7天每天测量PROTECT(选择性A1腺苷受体拮抗剂Rolofylline的安慰剂对照随机研究,用于住院的急性失代偿性心力衰竭患者)的血清钾浓度。容量超负荷以评估对充血和肾功能的治疗效果)试验。高钾血症定义为至少1次钾> 5.0 mEq / l。主要结局为180天全因死亡率。
结果
总体而言,血清钾浓度从基线时的4.3±0.6 mEq / l增加到出院或第7天时的4.5±0.6 mEq / l(p <0.001)。发生高钾血症的患者(n = 564; 35%)在住院之前更经常接受盐皮质激素拮抗剂(MRA)治疗,并且在住院期间更容易降低剂量,而不受混杂因素的影响。突发性高钾血症与不良预后无关。然而,无论发生何种高钾血症(p相互作用),住院期间MRA滴定与180天死亡率均独立相关(危险比[HR]:1.73; 95%置信区间[CI]:1.15至2.60)。> 0.10)。患有相同或增加剂量的MRA(HR:0.52; 95%CI:0.32至0.85)或血管紧张素转换酶(ACE)抑制剂/血管紧张素受体阻滞剂(ARB)出院的高钾血症患者(HR:0.47; 95 %CI:0.29至0.77)的180天死亡率较低。
结论
突发性高钾血症在因急性心力衰竭住院的患者中很常见,并且与不良后果无关。突发性高钾血症与MRA滴定有关,但在急性HF住院期间维持或增加MRA和/或ACE抑制剂/ ARB剂量的患者的180天生存期更好。










































 京公网安备 11010802027423号
京公网安备 11010802027423号