JACC: Heart Failure ( IF 10.3 ) Pub Date : 2019-09-30 , DOI: 10.1016/j.jchf.2019.07.008 Elke Platz 1 , Ross T Campbell 2 , Brian Claggett 3 , Eldrin F Lewis 3 , John D Groarke 3 , Kieran F Docherty 2 , Matthew M Y Lee 2 , Allison A Merz 1 , Montane Silverman 1 , Varsha Swamy 1 , Moritz Lindner 1 , Jose Rivero 3 , Scott D Solomon 3 , John J V McMurray 2
|
Objectives
This study sought to assess the prevalence, changes in, and prognostic importance of B-lines, a pulmonary congestion measure by using a simplified lung ultrasonography (LUS) method in acute heart failure (AHF).
Background
Pulmonary congestion is an important finding in AHF, but conventional methods for its detection are insensitive.
Methods
In a 2-site, prospective, observational study, 4-zone LUS was performed early during hospitalization for AHF (LUS1) and at discharge (LUS2). B-lines were quantified off-line, blinded to clinical findings and outcomes, by a core laboratory.
Results
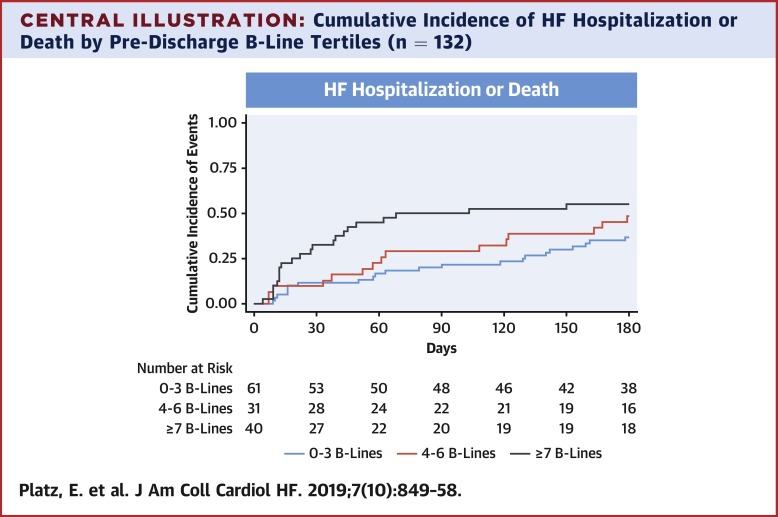
Among 349 patients (median, 75 years of age; 59% men; mean ejection fraction 39%), the sum of B-lines in 4 zones ranged from 0 to 18 (LUS1). The risk of an adverse in-hospital event increased with rising number of B-lines on LUS1: the odds ratio for each B-line tertile was 1.82 (95% confidence interval [CI]: 1.14 to 2.88; p = 0.011). B-line count decreased from a median of 6 (LUS1) to 4 (LUS2; p < 0.001) over 6 days (median). In 132 patients with LUS2 images, the risk of HF hospitalization or all-cause death was greater in patients with a higher number of B-lines at discharge. This relationship was stronger closer to discharge: unadjusted hazard ratio (HR) at 60 days was 3.30 (95% CI: 1.52 to 7.17; p = 0.002); 2.94 at 90 days (95% CI: 1.46 to 5.93; p = 0.003); and 2.01 at 180 days (95% CI: 1.11 to 3.64; p = 0.021). The association between number of B-lines and short- and long-term outcomes persisted after adjusting for important clinical variables, including N-terminal pro–B-type natriuretic peptide.
Conclusions
Pulmonary congestion using a simplified 4-zone LUS method was common in patients with AHF and improved with therapy. A higher number of B-lines at baseline and discharge identified patients at increased risk for adverse events.
中文翻译:
急性心力衰竭中的肺超声:肺充血的患病率和短期和长期结果。
目标
本研究旨在通过使用简化的肺超声 (LUS) 方法在急性心力衰竭 (AHF) 中评估 B 线的患病率、变化和预后重要性,B 线是一种肺淤血测量方法。
背景
肺充血是 AHF 的一个重要发现,但其检测的常规方法不敏感。
方法
在一项 2 地点、前瞻性、观察性研究中,4 区 LUS 在 AHF 住院期间 (LUS1) 和出院时 (LUS2) 早期进行。B 线由核心实验室离线量化,对临床发现和结果不知情。
结果
在 349 名患者(中位数,75 岁;59% 男性;平均射血分数 39%)中,4 个区域的 B 线总和范围从 0 到 18 (LUS1)。院内不良事件的风险随着 LUS1 上 B 线数量的增加而增加:每个 B 线三分位数的优势比为 1.82(95% 置信区间 [CI]:1.14 至 2.88;p = 0.011)。B 线计数在 6 天(中位数)内从 6 (LUS1) 的中位数减少到 4 (LUS2; p < 0.001)。在 132 名具有 LUS2 图像的患者中,出院时 B 线数量较多的患者发生 HF 住院或全因死亡的风险更高。这种关系在接近出院时更强:60 天时未调整的风险比 (HR) 为 3.30(95% CI:1.52 至 7.17;p = 0.002);90 天时为 2.94(95% CI:1.46 至 5.93;p = 0.003);180 天时为 2.01(95% CI:1.11 至 3.64;p = 0.021)。
结论
使用简化的 4 区 LUS 方法的肺充血在 AHF 患者中很常见,并且随着治疗得到改善。基线和出院时更多的 B 线确定了不良事件风险增加的患者。








































 京公网安备 11010802027423号
京公网安备 11010802027423号