Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: a prospective, cohort study.
The Lancet ( IF 98.4 ) Pub Date : 2019-09-27 , DOI: 10.1016/s0140-6736(19)31794-5 Ron Waksman 1 , Carlo Di Mario 2 , Rebecca Torguson 1 , Ziad A Ali 3 , Varinder Singh 4 , William H Skinner 5 , Andre K Artis 6 , Tim Ten Cate 7 , Eric Powers 8 , Christopher Kim 9 , Evelyn Regar 10 , S Chiu Wong 11 , Stephen Lewis 12 , Joanna Wykrzykowska 13 , Sandeep Dube 14 , Samer Kazziha 15 , Martin van der Ent 16 , Priti Shah 17 , Paige E Craig 1 , Quan Zou 1 , Paul Kolm 1 , H Bryan Brewer 1 , Hector M Garcia-Garcia 1 ,
The Lancet ( IF 98.4 ) Pub Date : 2019-09-27 , DOI: 10.1016/s0140-6736(19)31794-5 Ron Waksman 1 , Carlo Di Mario 2 , Rebecca Torguson 1 , Ziad A Ali 3 , Varinder Singh 4 , William H Skinner 5 , Andre K Artis 6 , Tim Ten Cate 7 , Eric Powers 8 , Christopher Kim 9 , Evelyn Regar 10 , S Chiu Wong 11 , Stephen Lewis 12 , Joanna Wykrzykowska 13 , Sandeep Dube 14 , Samer Kazziha 15 , Martin van der Ent 16 , Priti Shah 17 , Paige E Craig 1 , Quan Zou 1 , Paul Kolm 1 , H Bryan Brewer 1 , Hector M Garcia-Garcia 1 ,
Affiliation
|
BACKGROUND
Near-infrared spectroscopy (NIRS) intravascular ultrasound imaging can detect lipid-rich plaques (LRPs). LRPs are associated with acute coronary syndromes or myocardial infarction, which can result in revascularisation or cardiac death. In this study, we aimed to establish the relationship between LRPs detected by NIRS-intravascular ultrasound imaging at unstented sites and subsequent coronary events from new culprit lesions.
METHODS
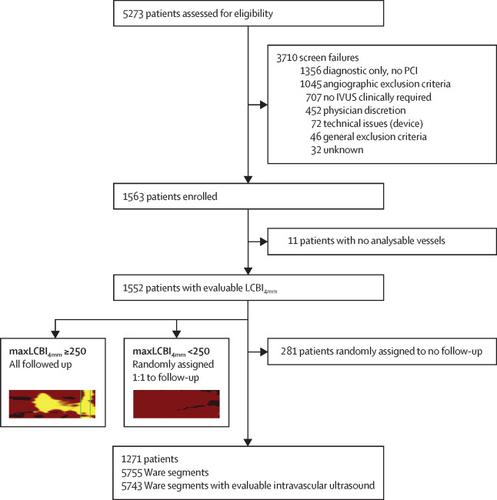
In this prospective, cohort study (LRP), patients from 44 medical centres were enrolled in Italy, Latvia, Netherlands, Slovakia, UK, and the USA. Patients with suspected coronary artery disease who underwent cardiac catheterisation with possible ad hoc percutaneous coronary intervention were eligible to be enrolled. Enrolled patients underwent scanning of non-culprit segments using NIRS-intravascular ultrasound imaging. The study had two hierarchal primary hypotheses, patient and plaque, each testing the association between maximum 4 mm Lipid Core Burden Index (maxLCBI4mm) and non-culprit major adverse cardiovascular events (NC-MACE). Enrolled patients with large LRPs (≥250 maxLCBI4mm) and a randomly selected half of patients with small LRPs (<250 maxLCBI4mm) were followed up for 24 months. This study is registered with ClinicalTrials.gov, NCT02033694.
FINDINGS
Between Feb 21, 2014, and March 30, 2016, 1563 patients were enrolled. NIRS-intravascular ultrasound device-related events were seen in six (0·4%) patients. 1271 patients (mean age 64 years, SD 10, 883 [69%] men, 388 [31%]women) with analysable maxLCBI4mm were allocated to follow-up. The 2-year cumulative incidence of NC-MACE was 9% (n=103). Both hierarchical primary hypotheses were met. On a patient level, the unadjusted hazard ratio (HR) for NC-MACE was 1·21 (95% CI 1·09-1·35; p=0·0004) for each 100-unit increase maxLCBI4mm) and adjusted HR 1·18 (1·05-1·32; p=0·0043). In patients with a maxLCBI4mm more than 400, the unadjusted HR for NC-MACE was 2·18 (1·48-3·22; p<0·0001) and adjusted HR was 1·89 (1·26-2·83; p=0·0021). At the plaque level, the unadjusted HR was 1·45 (1·30-1·60; p<0·0001) for each 100-unit increase in maxLCBI4mm. For segments with a maxLCBI4mm more than 400, the unadjusted HR for NC-MACE was 4·22 (2·39-7·45; p<0·0001) and adjusted HR was 3·39 (1·85-6·20; p<0·0001).
INTERPRETATION
NIRS imaging of non-obstructive territories in patients undergoing cardiac catheterisation and possible percutaneous coronary intervention was safe and can aid in identifying patients and segments at higher risk for subsequent NC-MACE. NIRS-intravascular ultrasound imaging adds to the armamentarium as the first diagnostic tool able to detect vulnerable patients and plaques in clinical practice.
FUNDING
Infraredx.
中文翻译:

近红外光谱法血管内超声成像识别易患冠心病的患者和斑块:一项前瞻性队列研究。
背景技术近红外光谱(NIRS)血管内超声成像可以检测富含脂质的斑块(LRP)。LRP与急性冠状动脉综合征或心肌梗塞有关,可能导致血运重建或心源性死亡。在这项研究中,我们旨在建立NIRS血管内超声成像在未支架位点检测到的LRP与随后的新罪魁祸首冠状动脉事件之间的关系。方法在这项前瞻性队列研究(LRP)中,来自44个医疗中心的患者纳入了意大利,拉脱维亚,荷兰,斯洛伐克,英国和美国。疑似冠状动脉疾病的患者接受了可能的特殊经皮冠状动脉介入治疗的心脏导管插入术后,才有资格入组。入组患者使用NIRS血管内超声成像进行非罪犯段扫描。该研究有两个层次的主要假设,即患者和斑块,每个假设检验最大4 mm脂质核心负担指数(maxLCBI4mm)与非罪魁祸首主要不良心血管事件(NC-MACE)之间的关联。入组大LRPs(≥250maxLCBI4mm)的患者和随机选择的半小LRPs(<250 maxLCBI4mm)的患者进行了24个月的随访。该研究已在ClinicalTrials.gov注册,NCT02033694。结果在2014年2月21日至2016年3月30日之间,共纳入1563例患者。在六名(0·4%)患者中发现了与NIRS血管内超声设备相关的事件。将1271例可分析的maxLCBI4mm患者(平均年龄64岁,SD 10,883名男性[69%],388名[31%]妇女)进行随访。NC-MACE的2年累积发生率为9%(n = 103)。两个层次的主要假设都得到了满足。在患者水平上,每增加100单位maxLCBI4mm,NC-MACE的未调整危险比(HR)为1·21(95%CI 1·09-1·35; p = 0·0004),并调整HR 1 ·18(1·05-1·32; p = 0·0043)。在maxLCBI4mm大于400的患者中,未调整的NC-MACE HR为2·18(1·48-3·22; p <0·0001),而调整后的HR为1·89(1·26-2·83) ; p = 0·0021)。在菌斑水平,maxLCBI4mm每增加100个单位,未调整的HR为1·45(1·30-1·60; p <0·0001)。对于maxLCBI4mm大于400的线段,NC-MACE的未调整HR为4·22(2·39-7·45; p <0·0001),调整后HR为3·39(1·85-6·20) ; p <0·0001)。解释在进行心脏导管插入术且可能进行经皮冠状动脉介入治疗的患者中,对非阻塞性领土进行NIRS成像是安全的,并且可以帮助识别较高风险的患者和进行后续NC-MACE的节段。NIRS血管内超声成像是装备库中的第一个诊断工具,能够在临床实践中检测出易受伤害的患者和斑块。资助红外线。
更新日期:2019-11-01
中文翻译:
近红外光谱法血管内超声成像识别易患冠心病的患者和斑块:一项前瞻性队列研究。
背景技术近红外光谱(NIRS)血管内超声成像可以检测富含脂质的斑块(LRP)。LRP与急性冠状动脉综合征或心肌梗塞有关,可能导致血运重建或心源性死亡。在这项研究中,我们旨在建立NIRS血管内超声成像在未支架位点检测到的LRP与随后的新罪魁祸首冠状动脉事件之间的关系。方法在这项前瞻性队列研究(LRP)中,来自44个医疗中心的患者纳入了意大利,拉脱维亚,荷兰,斯洛伐克,英国和美国。疑似冠状动脉疾病的患者接受了可能的特殊经皮冠状动脉介入治疗的心脏导管插入术后,才有资格入组。入组患者使用NIRS血管内超声成像进行非罪犯段扫描。该研究有两个层次的主要假设,即患者和斑块,每个假设检验最大4 mm脂质核心负担指数(maxLCBI4mm)与非罪魁祸首主要不良心血管事件(NC-MACE)之间的关联。入组大LRPs(≥250maxLCBI4mm)的患者和随机选择的半小LRPs(<250 maxLCBI4mm)的患者进行了24个月的随访。该研究已在ClinicalTrials.gov注册,NCT02033694。结果在2014年2月21日至2016年3月30日之间,共纳入1563例患者。在六名(0·4%)患者中发现了与NIRS血管内超声设备相关的事件。将1271例可分析的maxLCBI4mm患者(平均年龄64岁,SD 10,883名男性[69%],388名[31%]妇女)进行随访。NC-MACE的2年累积发生率为9%(n = 103)。两个层次的主要假设都得到了满足。在患者水平上,每增加100单位maxLCBI4mm,NC-MACE的未调整危险比(HR)为1·21(95%CI 1·09-1·35; p = 0·0004),并调整HR 1 ·18(1·05-1·32; p = 0·0043)。在maxLCBI4mm大于400的患者中,未调整的NC-MACE HR为2·18(1·48-3·22; p <0·0001),而调整后的HR为1·89(1·26-2·83) ; p = 0·0021)。在菌斑水平,maxLCBI4mm每增加100个单位,未调整的HR为1·45(1·30-1·60; p <0·0001)。对于maxLCBI4mm大于400的线段,NC-MACE的未调整HR为4·22(2·39-7·45; p <0·0001),调整后HR为3·39(1·85-6·20) ; p <0·0001)。解释在进行心脏导管插入术且可能进行经皮冠状动脉介入治疗的患者中,对非阻塞性领土进行NIRS成像是安全的,并且可以帮助识别较高风险的患者和进行后续NC-MACE的节段。NIRS血管内超声成像是装备库中的第一个诊断工具,能够在临床实践中检测出易受伤害的患者和斑块。资助红外线。










































 京公网安备 11010802027423号
京公网安备 11010802027423号