Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Association of Treatment With Metformin vs Sulfonylurea With Major Adverse Cardiovascular Events Among Patients With Diabetes and Reduced Kidney Function
JAMA ( IF 120.7 ) Pub Date : 2019-09-24 , DOI: 10.1001/jama.2019.13206 Christianne L Roumie 1, 2 , Jonathan Chipman 3 , Jea Young Min 1, 4 , Amber J Hackstadt 3 , Adriana M Hung 1, 2 , Robert A Greevy 3 , Carlos G Grijalva 1, 4 , Tom Elasy 1, 2 , Marie R Griffin 1, 2, 4
JAMA ( IF 120.7 ) Pub Date : 2019-09-24 , DOI: 10.1001/jama.2019.13206 Christianne L Roumie 1, 2 , Jonathan Chipman 3 , Jea Young Min 1, 4 , Amber J Hackstadt 3 , Adriana M Hung 1, 2 , Robert A Greevy 3 , Carlos G Grijalva 1, 4 , Tom Elasy 1, 2 , Marie R Griffin 1, 2, 4
Affiliation
|
Importance
Before 2016, safety concerns limited metformin use in patients with kidney disease; however, the effectiveness of metformin on clinical outcomes in patients with reduced kidney function remains unknown. Objective
To compare major adverse cardiovascular events (MACE) among patients with diabetes and reduced kidney function who continued treatment with metformin or a sulfonylurea. Design, Setting, and Participants
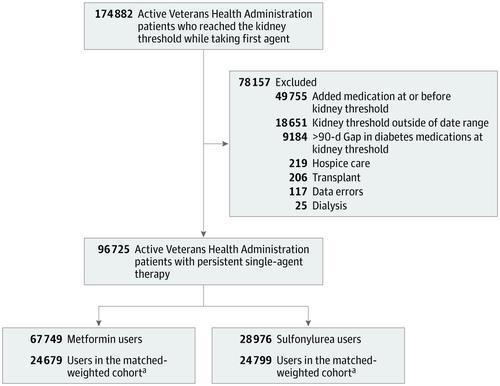
Retrospective cohort study of US veterans receiving care within the national Veterans Health Administration, with data supplemented by linkage to Medicare, Medicaid, and National Death Index data from 2001 through 2016. There were 174 882 persistent new users of metformin and sulfonylureas who reached a reduced kidney function threshold (estimated glomerular filtration rate <60 mL/min/1.73 m2 or creatinine ≥1.4 mg/dL for women or ≥1.5 mg/dL for men). Patients were followed up from reduced kidney function threshold until MACE, treatment change, loss to follow-up, death, or study end (December 2016). Exposures
New users of metformin or sulfonylurea monotherapy who continued treatment with their glucose-lowering medication after reaching reduced kidney function. Main Outcomes and Measures
MACE included hospitalization for acute myocardial infarction, stroke, transient ischemic attack, or cardiovascular death. The analyses used propensity score weighting to compare the cause-specific hazard of MACE between treatments and estimate cumulative risk accounting for the competing risks of changing therapy or noncardiovascular death. Results
There were 67 749 metformin and 28 976 sulfonylurea persistent monotherapy users; the weighted cohort included 24 679 metformin and 24 799 sulfonylurea users (median age, 70 years [interquartile range {IQR}, 62.8-77.8]; 48 497 men [98%]; and 40 476 white individuals [82%], with median estimated glomerular filtration rate of 55.8 mL/min/1.73 m2 [IQR, 51.6-58.2] and hemoglobin A1c level of 6.6% [IQR, 6.1%-7.2%] at cohort entry). During follow-up (median, 1.0 year for metformin vs 1.2 years for sulfonylurea), there were 1048 MACE outcomes (23.0 per 1000 person-years) among metformin users and 1394 events (29.2 per 1000 person-years) among sulfonylurea users. The cause-specific adjusted hazard ratio of MACE for metformin was 0.80 (95% CI, 0.75-0.86) compared with sulfonylureas, yielding an adjusted rate difference of 5.8 (95% CI, 4.1-7.3) fewer events per 1000 person-years of metformin use compared with sulfonylurea use. Conclusions and Relevance
Among patients with diabetes and reduced kidney function persisting with monotherapy, treatment with metformin, compared with a sulfonylurea, was associated with a lower risk of MACE.
中文翻译:

在糖尿病和肾功能下降患者中,二甲双胍与磺脲类药物治疗与主要心血管不良事件的相关性
重要性 2016 年之前,安全问题限制了二甲双胍在肾病患者中的使用;然而,二甲双胍对肾功能下降患者临床结果的有效性仍不清楚。目的比较继续使用二甲双胍或磺脲类药物治疗的糖尿病肾功能下降患者的主要不良心血管事件(MACE)。设计、设置和参与者对美国退伍军人在国家退伍军人健康管理局内接受护理的回顾性队列研究,数据通过与 2001 年至 2016 年的医疗保险、医疗补助和国家死亡指数数据的关联进行补充。二甲双胍有 174 882 名持续新用户和达到肾功能阈值降低的磺脲类药物(估计肾小球滤过率 <60 mL/min/1.73 m2 或肌酐≥1. 女性 4 mg/dL 或男性 ≥1.5 mg/dL)。从肾功能阈值降低到 MACE、治疗改变、失访、死亡或研究结束(2016 年 12 月)对患者进行随访。暴露 二甲双胍或磺脲类单药治疗的新用户在肾功能下降后继续使用降糖药物治疗。主要结果和措施 MACE 包括因急性心肌梗死、中风、短暂性脑缺血发作或心血管死亡而住院。分析使用倾向评分加权来比较治疗之间 MACE 的特定原因危害,并估计累积风险,以解释改变治疗或非心血管死亡的竞争风险。结果二甲双胍持续单药使用者67 749人,磺脲类药物持续单药使用者28 976人;加权队列包括 24 679 名二甲双胍和 24 799 名磺脲类药物使用者(中位年龄,70 岁 [四分位距 {IQR},62.8-77.8];48 497 名男性 [98%];和 40 476 名白人 [82%],中位年龄入组时估计肾小球滤过率为 55.8 mL/min/1.73 m2 [IQR,51.6-58.2],血红蛋白 A1c 水平为 6.6% [IQR,6.1%-7.2%]。在随访期间(中位值,二甲双胍组为 1.0 年,磺脲类药物为 1.2 年),二甲双胍使用者中有 1048 个 MACE 结果(23.0/1000 人年),而磺脲类药物使用者中有 1394 个事件(29.2/1000 人年)。与磺脲类药物相比,二甲双胍的原因特异性调整风险比为 0.80(95% CI,0.75-0.86),调整后的发生率差异为每 1000 人年事件减少 5.8(95% CI,4.1-7.3)。二甲双胍的使用与磺脲类的使用相比。
更新日期:2019-09-24
中文翻译:
在糖尿病和肾功能下降患者中,二甲双胍与磺脲类药物治疗与主要心血管不良事件的相关性
重要性 2016 年之前,安全问题限制了二甲双胍在肾病患者中的使用;然而,二甲双胍对肾功能下降患者临床结果的有效性仍不清楚。目的比较继续使用二甲双胍或磺脲类药物治疗的糖尿病肾功能下降患者的主要不良心血管事件(MACE)。设计、设置和参与者对美国退伍军人在国家退伍军人健康管理局内接受护理的回顾性队列研究,数据通过与 2001 年至 2016 年的医疗保险、医疗补助和国家死亡指数数据的关联进行补充。二甲双胍有 174 882 名持续新用户和达到肾功能阈值降低的磺脲类药物(估计肾小球滤过率 <60 mL/min/1.73 m2 或肌酐≥1. 女性 4 mg/dL 或男性 ≥1.5 mg/dL)。从肾功能阈值降低到 MACE、治疗改变、失访、死亡或研究结束(2016 年 12 月)对患者进行随访。暴露 二甲双胍或磺脲类单药治疗的新用户在肾功能下降后继续使用降糖药物治疗。主要结果和措施 MACE 包括因急性心肌梗死、中风、短暂性脑缺血发作或心血管死亡而住院。分析使用倾向评分加权来比较治疗之间 MACE 的特定原因危害,并估计累积风险,以解释改变治疗或非心血管死亡的竞争风险。结果二甲双胍持续单药使用者67 749人,磺脲类药物持续单药使用者28 976人;加权队列包括 24 679 名二甲双胍和 24 799 名磺脲类药物使用者(中位年龄,70 岁 [四分位距 {IQR},62.8-77.8];48 497 名男性 [98%];和 40 476 名白人 [82%],中位年龄入组时估计肾小球滤过率为 55.8 mL/min/1.73 m2 [IQR,51.6-58.2],血红蛋白 A1c 水平为 6.6% [IQR,6.1%-7.2%]。在随访期间(中位值,二甲双胍组为 1.0 年,磺脲类药物为 1.2 年),二甲双胍使用者中有 1048 个 MACE 结果(23.0/1000 人年),而磺脲类药物使用者中有 1394 个事件(29.2/1000 人年)。与磺脲类药物相比,二甲双胍的原因特异性调整风险比为 0.80(95% CI,0.75-0.86),调整后的发生率差异为每 1000 人年事件减少 5.8(95% CI,4.1-7.3)。二甲双胍的使用与磺脲类的使用相比。


























 京公网安备 11010802027423号
京公网安备 11010802027423号