Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
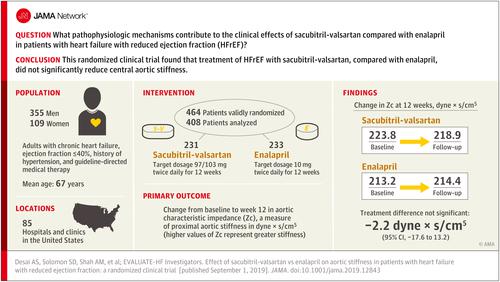
Effect of Sacubitril-Valsartan vs Enalapril on Aortic Stiffness in Patients With Heart Failure and Reduced Ejection Fraction
JAMA ( IF 63.1 ) Pub Date : 2019-09-17 , DOI: 10.1001/jama.2019.12843 Akshay S Desai 1 , Scott D Solomon 1 , Amil M Shah 1 , Brian L Claggett 1 , James C Fang 2 , Joseph Izzo 3 , Kevin McCague 4 , Cheryl A Abbas 4 , Ricardo Rocha 4 , Gary F Mitchell 5 ,
JAMA ( IF 63.1 ) Pub Date : 2019-09-17 , DOI: 10.1001/jama.2019.12843 Akshay S Desai 1 , Scott D Solomon 1 , Amil M Shah 1 , Brian L Claggett 1 , James C Fang 2 , Joseph Izzo 3 , Kevin McCague 4 , Cheryl A Abbas 4 , Ricardo Rocha 4 , Gary F Mitchell 5 ,
Affiliation
|
Importance
Compared with enalapril, sacubitril-valsartan reduces cardiovascular mortality and heart failure hospitalization in patients with heart failure and reduced ejection fraction (HFrEF). These benefits may be related to effects on hemodynamics and cardiac remodeling. Objective
To determine whether treatment of HFrEF with sacubitril-valsartan improves central aortic stiffness and cardiac remodeling compared with enalapril. Design, Setting, and Participants
Randomized, double-blind clinical trial of 464 participants with heart failure and ejection fraction of 40% or less enrolled across 85 US sites between August 17, 2016, and June 28, 2018. Follow-up was completed on January 26, 2019. Interventions
Randomization (1:1) to sacubitril-valsartan (n = 231; target dosage, 97/103 mg twice daily) vs enalapril (n = 233; target dosage, 10 mg twice daily) for 12 weeks. Main Outcomes and Measures
The primary outcome was change from baseline to week 12 in aortic characteristic impedance (Zc), a measure of central aortic stiffness. Prespecified secondary outcomes included change from baseline to week 12 in N-terminal pro-B-type natriuretic peptide, ejection fraction, global longitudinal strain, mitral annular relaxation velocity, mitral E/e' ratio, left ventricular end-systolic and end-diastolic volume indexes (LVESVI and LVEDVI), left atrial volume index, and ventricular-vascular coupling ratio. Results
Of 464 validly randomized participants (mean age, 67.3 [SD, 9.1] years; 23.5% women), 427 completed the study. At 12 weeks, Zc decreased from 223.8 to 218.9 dyne × s/cm5 in the sacubitril-valsartan group and increased from 213.2 to 214.4 dyne × s/cm5 in the enalapril group (treatment difference, -2.2 [95% CI, -17.6 to 13.2] dyne × s/cm5; P = .78). Of 9 prespecified secondary end points, no significant between-group difference in change from baseline was seen in 4, including left ventricular ejection fraction (34%-36% with sacubitril-valsartan vs 33 to 35% with enalapril; treatment difference, 0.6% [95% CI, -0.4% to 1.7%]; P = .24). However, greater reductions from baseline were seen with sacubitril-valsartan than with enalapril in all others, including left atrial volume (from 30.4 mL/m2 to 28.2 mL/m2 vs from 29.8 mL/m2 to 30.5 mL/m2; treatment difference, -2.8 mL/m2 [95% CI, -4.0 to -1.6 mL/m2]; P < .001), LVEDVI (from 75.1 mL/m2 to 70.3 mL/m2 vs from 79.1 mL/m2 to 75.6 mL/m2; treatment difference, -2.0 mL/m2 [95% CI, -3.7 to 0.3 mL/m2]; P = .02), LVESVI (from 50.8 mL/m2 to 46.3 mL/m2 vs from 54.1 to 50.6 mL/m2; treatment difference, -1.6 mL/m2 [95% CI, -3.1 to -0.03 mL/m2]; P = .045), and mitral E/e' ratio (from 13.8 to 12.3 vs from 13.4 to 13.8; treatment difference, -1.8 [95% CI, -2.8 to -0.8]; P = .001). Rates of adverse events including hypotension (1.7% vs 3.9%) were similar in both groups. Conclusions and Relevance
Treatment of HFrEF with sacubitril-valsartan, compared with enalapril, did not significantly reduce central aortic stiffness. The study findings may provide insight into mechanisms underlying the effects of sacubitril-valsartan in HFrEF. Trial Registration
ClinicalTrials.gov Identifier: NCT02874794.
中文翻译:

沙库巴曲缬沙坦与依那普利对心力衰竭和射血分数降低患者主动脉僵硬的影响
重要性 与依那普利相比,沙库巴曲缬沙坦可降低心力衰竭和射血分数降低 (HFrEF) 患者的心血管死亡率和心力衰竭住院率。这些益处可能与对血流动力学和心脏重塑的影响有关。目的 确定与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 是否能改善中心主动脉僵硬度和心脏重构。设计、设置和参与者 2016 年 8 月 17 日至 2018 年 6 月 28 日期间,在美国 85 个地点招募了 464 名心力衰竭和射血分数为 40% 或以下的参与者的随机双盲临床试验。随访完成于2019 年 1 月 26 日。随机化 (1:1) 到沙库巴曲缬沙坦(n = 231;目标剂量,97/103 mg,每天两次)与依那普利(n = 233;目标剂量,10 毫克,每天两次),持续 12 周。主要结果和测量 主要结果是主动脉特征阻抗 (Zc) 从基线到第 12 周的变化,这是一种测量中心主动脉僵硬度的方法。预先设定的次要结果包括从基线到第 12 周的 N 末端前 B 型利钠肽、射血分数、整体纵向应变、二尖瓣环松弛速度、二尖瓣 E/e' 比、左心室收缩末期和舒张末期的变化容积指数(LVESVI 和 LVEDVI)、左心房容积指数和心室-血管耦合比。结果 在 464 名有效随机参与者(平均年龄 67.3 [SD,9.1] 岁;23.5% 女性)中,427 人完成了研究。12 周时,沙库巴曲缬沙坦组的 Zc 从 223.8 下降到 218.9 dyne × s/cm5,从 213.2 上升到 214。依那普利组为 4 dyne × s/cm5(治疗差异,-2.2 [95% CI,-17.6 至 13.2] dyne × s/cm5;P = .78)。在 9 个预先设定的次要终点中,4 个未观察到与基线相比的显着组间变化,包括左心室射血分数(沙库巴曲缬沙坦组为 34%-36%,依那普利组为 33% 至 35%;治疗差异为 0.6% [95% CI,-0.4% 至 1.7%];P = .24)。然而,在包括左心房容量在内的所有其他方面,沙库巴曲缬沙坦与依那普利相比,从基线的减少幅度更大(从 30.4 mL/m2 到 28.2 mL/m2 对比从 29.8 mL/m2 到 30.5 mL/m2;治疗差异,- 2.8 mL/m2 [95% CI,-4.0 至 -1.6 mL/m2];P < .001),LVEDVI(从 75.1 mL/m2 至 70.3 mL/m2 对比从 79.1 mL/m2 至 75.6 mL/m2;治疗差异,-2.0 mL/m2 [95% CI,-3.7 至 0.3 mL/m2];P = .02),LVESVI(从 50. 8 mL/m2 至 46.3 mL/m2 对比 54.1 至 50.6 mL/m2;处理差异,-1.6 mL/m2 [95% CI,-3.1 至 -0.03 mL/m2];P = .045)和二尖瓣 E/e' 比值(从 13.8 到 12.3 对比从 13.4 到 13.8;治疗差异,-1.8 [95% CI,-2.8 到 -0.8];P = .001)。包括低血压在内的不良事件发生率(1.7% vs 3.9%)在两组中相似。结论和相关性 与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 并未显着降低中心主动脉僵硬度。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。治疗差异,-1.8 [95% CI,-2.8 至 -0.8];P = .001)。包括低血压在内的不良事件发生率(1.7% vs 3.9%)在两组中相似。结论和相关性 与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 并未显着降低中心主动脉僵硬度。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。治疗差异,-1.8 [95% CI,-2.8 至 -0.8];P = .001)。包括低血压在内的不良事件发生率(1.7% vs 3.9%)在两组中相似。结论和相关性 与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 并未显着降低中心主动脉僵硬度。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。
更新日期:2019-09-17
中文翻译:
沙库巴曲缬沙坦与依那普利对心力衰竭和射血分数降低患者主动脉僵硬的影响
重要性 与依那普利相比,沙库巴曲缬沙坦可降低心力衰竭和射血分数降低 (HFrEF) 患者的心血管死亡率和心力衰竭住院率。这些益处可能与对血流动力学和心脏重塑的影响有关。目的 确定与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 是否能改善中心主动脉僵硬度和心脏重构。设计、设置和参与者 2016 年 8 月 17 日至 2018 年 6 月 28 日期间,在美国 85 个地点招募了 464 名心力衰竭和射血分数为 40% 或以下的参与者的随机双盲临床试验。随访完成于2019 年 1 月 26 日。随机化 (1:1) 到沙库巴曲缬沙坦(n = 231;目标剂量,97/103 mg,每天两次)与依那普利(n = 233;目标剂量,10 毫克,每天两次),持续 12 周。主要结果和测量 主要结果是主动脉特征阻抗 (Zc) 从基线到第 12 周的变化,这是一种测量中心主动脉僵硬度的方法。预先设定的次要结果包括从基线到第 12 周的 N 末端前 B 型利钠肽、射血分数、整体纵向应变、二尖瓣环松弛速度、二尖瓣 E/e' 比、左心室收缩末期和舒张末期的变化容积指数(LVESVI 和 LVEDVI)、左心房容积指数和心室-血管耦合比。结果 在 464 名有效随机参与者(平均年龄 67.3 [SD,9.1] 岁;23.5% 女性)中,427 人完成了研究。12 周时,沙库巴曲缬沙坦组的 Zc 从 223.8 下降到 218.9 dyne × s/cm5,从 213.2 上升到 214。依那普利组为 4 dyne × s/cm5(治疗差异,-2.2 [95% CI,-17.6 至 13.2] dyne × s/cm5;P = .78)。在 9 个预先设定的次要终点中,4 个未观察到与基线相比的显着组间变化,包括左心室射血分数(沙库巴曲缬沙坦组为 34%-36%,依那普利组为 33% 至 35%;治疗差异为 0.6% [95% CI,-0.4% 至 1.7%];P = .24)。然而,在包括左心房容量在内的所有其他方面,沙库巴曲缬沙坦与依那普利相比,从基线的减少幅度更大(从 30.4 mL/m2 到 28.2 mL/m2 对比从 29.8 mL/m2 到 30.5 mL/m2;治疗差异,- 2.8 mL/m2 [95% CI,-4.0 至 -1.6 mL/m2];P < .001),LVEDVI(从 75.1 mL/m2 至 70.3 mL/m2 对比从 79.1 mL/m2 至 75.6 mL/m2;治疗差异,-2.0 mL/m2 [95% CI,-3.7 至 0.3 mL/m2];P = .02),LVESVI(从 50. 8 mL/m2 至 46.3 mL/m2 对比 54.1 至 50.6 mL/m2;处理差异,-1.6 mL/m2 [95% CI,-3.1 至 -0.03 mL/m2];P = .045)和二尖瓣 E/e' 比值(从 13.8 到 12.3 对比从 13.4 到 13.8;治疗差异,-1.8 [95% CI,-2.8 到 -0.8];P = .001)。包括低血压在内的不良事件发生率(1.7% vs 3.9%)在两组中相似。结论和相关性 与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 并未显着降低中心主动脉僵硬度。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。治疗差异,-1.8 [95% CI,-2.8 至 -0.8];P = .001)。包括低血压在内的不良事件发生率(1.7% vs 3.9%)在两组中相似。结论和相关性 与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 并未显着降低中心主动脉僵硬度。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。治疗差异,-1.8 [95% CI,-2.8 至 -0.8];P = .001)。包括低血压在内的不良事件发生率(1.7% vs 3.9%)在两组中相似。结论和相关性 与依那普利相比,沙库巴曲缬沙坦治疗 HFrEF 并未显着降低中心主动脉僵硬度。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。研究结果可能有助于深入了解沙库巴曲缬沙坦在 HFrEF 中的作用机制。试验注册 ClinicalTrials.gov 标识符:NCT02874794。






































 京公网安备 11010802027423号
京公网安备 11010802027423号