当前位置:
X-MOL 学术
›
Gastroenterology
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Clip Closure After Resection of Large Colorectal Lesions With Substantial Risk of Bleeding.
Gastroenterology ( IF 25.7 ) Pub Date : 2019-07-27 , DOI: 10.1053/j.gastro.2019.07.037 Eduardo Albéniz 1 , Marco Antonio Álvarez 2 , Jorge C Espinós 3 , Oscar Nogales 4 , Carlos Guarner 5 , Pedro Alonso 6 , Manuel Rodríguez-Téllez 7 , Alberto Herreros de Tejada 8 , José Santiago 8 , Marco Bustamante-Balén 9 , Joaquín Rodríguez Sánchez 10 , Felipe Ramos-Zabala 11 , Eduardo Valdivielso 6 , Felipe Martínez-Alcalá 12 , María Fraile 13 , Alfonso Elosua 1 , María Fernanda Guerra Veloz 7 , Berta Ibáñez Beroiz 14 , Ferrán Capdevila 15 , Mónica Enguita-Germán 15
Gastroenterology ( IF 25.7 ) Pub Date : 2019-07-27 , DOI: 10.1053/j.gastro.2019.07.037 Eduardo Albéniz 1 , Marco Antonio Álvarez 2 , Jorge C Espinós 3 , Oscar Nogales 4 , Carlos Guarner 5 , Pedro Alonso 6 , Manuel Rodríguez-Téllez 7 , Alberto Herreros de Tejada 8 , José Santiago 8 , Marco Bustamante-Balén 9 , Joaquín Rodríguez Sánchez 10 , Felipe Ramos-Zabala 11 , Eduardo Valdivielso 6 , Felipe Martínez-Alcalá 12 , María Fraile 13 , Alfonso Elosua 1 , María Fernanda Guerra Veloz 7 , Berta Ibáñez Beroiz 14 , Ferrán Capdevila 15 , Mónica Enguita-Germán 15
Affiliation
|
BACKGROUND & AIMS
It is not clear whether closure of mucosal defects with clips after colonic endoscopic mucosal resection (EMR) prevents delayed bleeding, although it seems to have no protective effects when risk is low. We performed a randomized trial to evaluate the efficacy of complete clip closure of large (≥2 cm) nonpedunculated colorectal lesions after EMR in patients with an estimated average or high risk of delayed bleeding.
METHODS
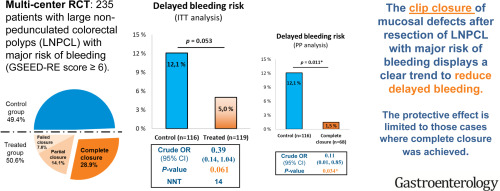
We performed a single-blind trial at 11 hospitals in Spain from May 2016 through June 2018, including 235 consecutive patients who underwent EMR for large nonpedunculated colorectal lesions with an average or high risk of delayed bleeding (based on Spanish Endoscopy Society Endoscopic Resection Group score). Participants were randomly assigned to groups that received closure of the scar with 11-mm through-the-scope clips (treated, n = 119) or no clip (control, n = 116). The primary outcome was proportion of patients in each group with delayed bleeding, defined as evident hematochezia that required medical intervention within 15 days after colonoscopy.
RESULTS
In the clip group, complete closure was achieved in 68 (57%) cases, with partial closure in 33 (28%) cases and failure to close in 18 (15%) cases. Delayed bleeding occurred in 14 (12.1%) patients in the control group and in 6 (5%) patients in the clip group (absolute risk difference, reduction of 7% in the clip group; 95% confidence interval, -14.7% to 0.3%). After completion of the clip closure, there was only 1 (1.5%) case of delayed bleeding (absolute risk difference, reduction of 10.6%; 95% confidence interval, -4.3% to 17.9%).
CONCLUSIONS
In a randomized trial of patients with large nonpedunculated colorectal lesions undergoing EMR, we found that clip closure of mucosal defects in patients with a risk of bleeding can be a challenge, but also reduces delayed bleeding. Prevention of delayed bleeding required complete clip closure. ClinicalTrials.gov ID: NCT02765022.
中文翻译:

大型结直肠癌切除后夹子闭合,有大量出血的危险。
背景与目的目前尚不清楚结肠内窥镜黏膜切除术(EMR)后用夹子闭合黏膜缺损是否可以防止延迟出血,尽管在低风险时似乎没有保护作用。我们进行了一项随机试验,以评估EMR后大(≥2 cm)无蒂大肠癌病灶完全夹子闭合对估计平均或高风险延迟出血患者的疗效。方法我们于2016年5月至2018年6月在西班牙的11家医院进行了单盲试验,包括235例因大而无蒂的大肠直肠病变接受EMR的平均或高延迟出血风险接受EMR的患者(根据西班牙内窥镜协会内镜切除组分数)。参与者被随机分配到使用11毫米的镜下夹子(治疗,n = 119)或无夹子(对照组,n = 116)闭合疤痕的组。主要结局是每组延迟出血的患者比例,出血定义为结肠镜检查后15天内需要医疗干预的明显便血。结果在夹子组中,有68例(57%)完全闭合,其中33例(28%)局部闭合,18例(15%)没有闭合。对照组中14例(12.1%)患者和夹子组6例(5%)患者发生延迟出血(绝对风险差异,夹子组减少7%; 95%置信区间为-14.7%至0.3 %)。夹子闭合完成后,只有1例(1.5%)延迟出血(绝对危险性差异,减少了10.6%;仅发生了3次)。95%置信区间,-4.3%至17.9%)。结论在接受大剂量未切除大肠病变的患者进行EMR的随机试验中,我们发现有出血风险的患者黏膜缺损的夹子闭合可能是一个挑战,但也可以减少延迟出血。为防止延迟出血,需要完全闭合夹子。ClinicalTrials.gov ID:NCT02765022。
更新日期:2019-11-18
中文翻译:
大型结直肠癌切除后夹子闭合,有大量出血的危险。
背景与目的目前尚不清楚结肠内窥镜黏膜切除术(EMR)后用夹子闭合黏膜缺损是否可以防止延迟出血,尽管在低风险时似乎没有保护作用。我们进行了一项随机试验,以评估EMR后大(≥2 cm)无蒂大肠癌病灶完全夹子闭合对估计平均或高风险延迟出血患者的疗效。方法我们于2016年5月至2018年6月在西班牙的11家医院进行了单盲试验,包括235例因大而无蒂的大肠直肠病变接受EMR的平均或高延迟出血风险接受EMR的患者(根据西班牙内窥镜协会内镜切除组分数)。参与者被随机分配到使用11毫米的镜下夹子(治疗,n = 119)或无夹子(对照组,n = 116)闭合疤痕的组。主要结局是每组延迟出血的患者比例,出血定义为结肠镜检查后15天内需要医疗干预的明显便血。结果在夹子组中,有68例(57%)完全闭合,其中33例(28%)局部闭合,18例(15%)没有闭合。对照组中14例(12.1%)患者和夹子组6例(5%)患者发生延迟出血(绝对风险差异,夹子组减少7%; 95%置信区间为-14.7%至0.3 %)。夹子闭合完成后,只有1例(1.5%)延迟出血(绝对危险性差异,减少了10.6%;仅发生了3次)。95%置信区间,-4.3%至17.9%)。结论在接受大剂量未切除大肠病变的患者进行EMR的随机试验中,我们发现有出血风险的患者黏膜缺损的夹子闭合可能是一个挑战,但也可以减少延迟出血。为防止延迟出血,需要完全闭合夹子。ClinicalTrials.gov ID:NCT02765022。










































 京公网安备 11010802027423号
京公网安备 11010802027423号