当前位置:
X-MOL 学术
›
Gastroenterology
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Increased Risk for Hepatocellular Carcinoma Persists Up to 10 Years After HCV Eradication in Patients With Baseline Cirrhosis or High FIB-4 Scores.
Gastroenterology ( IF 25.7 ) Pub Date : 2019-07-26 , DOI: 10.1053/j.gastro.2019.07.033 George N Ioannou 1 , Lauren A Beste 2 , Pamela K Green 3 , Amit G Singal 4 , Elliot B Tapper 5 , Akbar K Waljee 5 , Richard K Sterling 6 , Jordan J Feld 7 , David E Kaplan 8 , Tamar H Taddei 9 , Kristin Berry 3
Gastroenterology ( IF 25.7 ) Pub Date : 2019-07-26 , DOI: 10.1053/j.gastro.2019.07.033 George N Ioannou 1 , Lauren A Beste 2 , Pamela K Green 3 , Amit G Singal 4 , Elliot B Tapper 5 , Akbar K Waljee 5 , Richard K Sterling 6 , Jordan J Feld 7 , David E Kaplan 8 , Tamar H Taddei 9 , Kristin Berry 3
Affiliation
|
BACKGROUND & AIMS
It is unclear if hepatocellular carcinoma (HCC) risk declines over time after hepatitis C virus (HCV) eradication. We analyzed changes in HCC annual incidence over time following HCV eradication and identified dynamic markers of HCC risk.
METHODS
We identified 48,135 patients who initiated HCV antiviral treatment from 2000 through 2015 and achieved a sustained virologic response (SVR) in the Veterans Health Administration (29,033 treated with direct-acting antiviral [DAA] agents and 19,102 treated with interferon-based regimens). Patients were followed after treatment until February 14, 2019 (average 5.4 years), during which 1509 incident HCCs were identified.
RESULTS
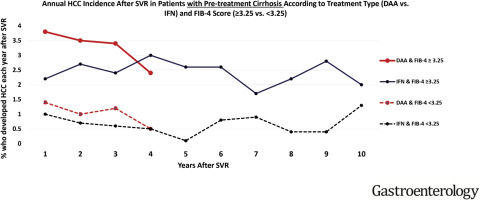
Among patients with cirrhosis before treatment with DAAs (n = 9784), those with pre-SVR fibrosis-4 (FIB-4) scores ≥3.25 had a higher annual incidence of HCC (3.66%/year) than those with FIB-4 scores <3.25 (1.16%/year) (adjusted hazard ratio 2.14; 95% confidence interval 1.66-2.75). In DAA-treated patients with cirrhosis and FIB-4 scores ≥3.25, annual HCC risk decreased from 3.8%/year in the first year after SVR to 2.4%/year by the fourth year (P=.01). In interferon-treated patients with FIB-4 scores ≥3.25, annual HCC risk remained above 2%/year, even 10 years after SVR. A decrease in FIB-4 scores from ≥3.25 pre-SVR to <3.25 post-SVR was associated with an approximately 50% lower risk of HCC, but the absolute annual risk remained above 2%/year. Patients without cirrhosis before treatment (n = 38,351) had a low risk of HCC, except for those with pre-SVR FIB-4 scores ≥3.25 (HCC risk 1.22%/year) and post-SVR FIB-4 scores ≥3.25 (HCC risk 2.39%/year); risk remained high for many years after SVR.
CONCLUSIONS
Patients with cirrhosis before an SVR to treatment for HCV infection continue to have a high risk for HCC (>2%/year) for many years, even if their FIB-4 score decreases, and should continue surveillance. Patients without cirrhosis but with FIB-4 scores ≥3.25 have a high enough risk to merit HCC surveillance, especially if FIB-4 remains ≥3.25 post-SVR.
中文翻译:

基线肝硬化或高FIB-4评分的患者在HCV根除后长达10年的肝细胞癌风险增加。
背景与目的目前尚不清楚在消灭丙型肝炎病毒(HCV)后,肝细胞癌(HCC)的风险是否会随时间下降。我们分析了HCV根除后随时间推移HCC年发病率的变化,并确定了HCC风险的动态标志。方法我们确定了48,135例从2000年至2015年开始进行HCV抗病毒治疗并在退伍军人卫生管理局中实现持续病毒学应答(SVR)的患者(29,033例接受直接作用抗病毒[DAA]药物治疗,19,102例接受基于干扰素的治疗方案)。治疗后对患者进行随访,直到2019年2月14日(平均5.4年),在此期间确定了1509例HCC事件。结果在接受DAA治疗的肝硬化患者中(n = 9784),SVR前纤维化4(FIB-4)评分≥3的患者。25例肝癌的年发生率(3.66%/年)高于FIB-4分数<3.25(1.16%/年)的人(校正风险比2.14; 95%置信区间1.66-2.75)。在接受DAA治疗的肝硬化且FIB-4得分≥3.25的患者中,年HCC风险从SVR后的第一年的3.8%/年降低到第四年的2.4%/年(P = .01)。在FIB-4评分≥3.25的经干扰素治疗的患者中,即使在SVR后10年,每年的HCC风险仍高于2%/年。FIB-4评分从SVR之前的3.25降低到SVR之后的<3.25降低了大约50%的HCC风险,但绝对年度风险仍高于2%/年。治疗前无肝硬化的患者(n = 38,351)除SVR前FIB-4评分≥3.25(HCC风险为1.22%/年)和SVR FIB-4后评分≥3.25(HCC)的患者以外,均具有较低的HCC风险。风险为2.39%/年);SVR后的许多年中,风险仍然很高。结论在接受SVR治疗HCV感染之前的肝硬化患者,即使FIB-4评分降低,多年来仍继续存在HCC的高风险(> 2%/年),并应继续进行监测。无肝硬化但FIB-4评分≥3.25的患者有足够的风险进行HCC监测,尤其是在SVR后FIB-4仍≥3.25的情况下。
更新日期:2019-11-18
中文翻译:
基线肝硬化或高FIB-4评分的患者在HCV根除后长达10年的肝细胞癌风险增加。
背景与目的目前尚不清楚在消灭丙型肝炎病毒(HCV)后,肝细胞癌(HCC)的风险是否会随时间下降。我们分析了HCV根除后随时间推移HCC年发病率的变化,并确定了HCC风险的动态标志。方法我们确定了48,135例从2000年至2015年开始进行HCV抗病毒治疗并在退伍军人卫生管理局中实现持续病毒学应答(SVR)的患者(29,033例接受直接作用抗病毒[DAA]药物治疗,19,102例接受基于干扰素的治疗方案)。治疗后对患者进行随访,直到2019年2月14日(平均5.4年),在此期间确定了1509例HCC事件。结果在接受DAA治疗的肝硬化患者中(n = 9784),SVR前纤维化4(FIB-4)评分≥3的患者。25例肝癌的年发生率(3.66%/年)高于FIB-4分数<3.25(1.16%/年)的人(校正风险比2.14; 95%置信区间1.66-2.75)。在接受DAA治疗的肝硬化且FIB-4得分≥3.25的患者中,年HCC风险从SVR后的第一年的3.8%/年降低到第四年的2.4%/年(P = .01)。在FIB-4评分≥3.25的经干扰素治疗的患者中,即使在SVR后10年,每年的HCC风险仍高于2%/年。FIB-4评分从SVR之前的3.25降低到SVR之后的<3.25降低了大约50%的HCC风险,但绝对年度风险仍高于2%/年。治疗前无肝硬化的患者(n = 38,351)除SVR前FIB-4评分≥3.25(HCC风险为1.22%/年)和SVR FIB-4后评分≥3.25(HCC)的患者以外,均具有较低的HCC风险。风险为2.39%/年);SVR后的许多年中,风险仍然很高。结论在接受SVR治疗HCV感染之前的肝硬化患者,即使FIB-4评分降低,多年来仍继续存在HCC的高风险(> 2%/年),并应继续进行监测。无肝硬化但FIB-4评分≥3.25的患者有足够的风险进行HCC监测,尤其是在SVR后FIB-4仍≥3.25的情况下。










































 京公网安备 11010802027423号
京公网安备 11010802027423号