Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Eligibility and subsequent burden of cardiovascular disease of four strategies for blood pressure-lowering treatment: a retrospective cohort study
The Lancet ( IF 98.4 ) Pub Date : 2019-07-25 , DOI: 10.1016/s0140-6736(19)31359-5 Emily Herrett 1 , Sarah Gadd 1 , Rod Jackson 2 , Krishnan Bhaskaran 1 , Elizabeth Williamson 3 , Tjeerd van Staa 4 , Reecha Sofat 5 , Adam Timmis 6 , Liam Smeeth 7
中文翻译:

四种降压治疗策略的资格和随后的心血管疾病负担:一项回顾性队列研究
尽管有强有力的证据表明,在整个血压范围内的患者中都观察到了降低血压的益处,但全球范围内降低血压的治疗建议仍然主要以血压阈值为指导。在这项研究中,我们旨在以英国为例,调查提供血压治疗的替代策略的影响。
我们对 30-79 岁无心血管疾病的初级保健患者进行了一项回顾性队列研究,使用的数据来自与医院发病统计和国家统计局死亡率相关的英国临床实践研究数据链。我们评估和比较了四种不同的策略来确定治疗资格:使用 2011 年英国国家健康与护理卓越研究所 (NICE) 指南,或提议的 2019 年 NICE 指南,或单独血压(阈值≥140/90 mm Hg),或预测仅 10 年心血管风险(QRISK2 评分≥10%)。对患者进行随访,直至最早发生心血管疾病诊断、死亡或随访期结束(2016 年 3 月 31 日)。对于每种策略,我们估计了符合治疗条件的患者比例以及可以通过治疗预防的心血管事件的数量。然后,我们估计了英国普通人群的资格和 10 年内将发生的事件数量。
2011年1月1日至2016年3月31日期间,队列中的1 222 670名患者接受了中位随访4·3年(IQR 2·5–5·2)。根据 2011 年 NICE 指南,有 271 963 名患者 (22·2%) 有资格接受治疗;根据 2019 年 NICE 指南,有 327 429 名患者 (26·8%) 符合治疗资格;根据血压阈值,有 481 859 名患者 (39·4%) 有资格接受治疗140/90 mm Hg 或更高,以及 357 840 (29·3%)(基于 10% 或更高的 QRISK2 阈值)。随访期间,32 183 名患者被诊断患有心血管疾病(总体发病率为每 1000 人年 7·1,95% CI 7·0–7·2)。根据 2011 年 NICE 指南,符合每种策略的患者的心血管事件发生率为每 1000 人年 15·2 例(95% CI 15·0–15·5),根据 2011 年 NICE 指南,每 1000 人年为 14·9(14·7–15·1)。提出的 2019 年 NICE 指南,11·4 (11·3–11·6) 仅包含血压阈值,16·9 (16·7–17·1) 仅包含 QRISK2 阈值。根据英国人口规模,我们估计根据 2011 年 NICE 指南可以避免 233 152 起事件(28 名患者需要治疗 10 年才能避免一件事件),根据 2019 年 NICE 指南(29 名患者)可以避免 270 233 起事件,使用 2019 年 NICE 指南可以避免 301 523 起事件。血压阈值(38 名患者),以及 322 921 使用 QRISK2 阈值(27 名患者)。
基于心血管风险的策略(QRISK2≥10%)可以比 2011 年 NICE 指南多预防三分之一以上的心血管疾病事件,比 2019 年 NICE 指南多五分之一,并且在每次避免事件的治疗数量方面具有相似的效率。
国家健康研究所。
更新日期:2019-08-23
The Lancet ( IF 98.4 ) Pub Date : 2019-07-25 , DOI: 10.1016/s0140-6736(19)31359-5 Emily Herrett 1 , Sarah Gadd 1 , Rod Jackson 2 , Krishnan Bhaskaran 1 , Elizabeth Williamson 3 , Tjeerd van Staa 4 , Reecha Sofat 5 , Adam Timmis 6 , Liam Smeeth 7
Affiliation
|
Background
Worldwide treatment recommendations for lowering blood pressure continue to be guided predominantly by blood pressure thresholds, despite strong evidence that the benefits of blood pressure reduction are observed in patients across the blood pressure spectrum. In this study, we aimed to investigate the implications of alternative strategies for offering blood pressure treatment, using the UK as an illustrative example.Methods
We did a retrospective cohort study in primary care patients aged 30–79 years without cardiovascular disease, using data from the UK's Clinical Practice Research Datalink linked to Hospital Episode Statistics and Office for National Statistics mortality. We assessed and compared four different strategies to determine eligibility for treatment: using 2011 UK National Institute for Health and Care Excellence (NICE) guideline, or proposed 2019 NICE guideline, or blood pressure alone (threshold ≥140/90 mm Hg), or predicted 10-year cardiovascular risk alone (QRISK2 score ≥10%). Patients were followed up until the earliest occurrence of a cardiovascular disease diagnosis, death, or end of follow-up period (March 31, 2016). For each strategy, we estimated the proportion of patients eligible for treatment and number of cardiovascular events that could be prevented with treatment. We then estimated eligibility and number of events that would occur during 10 years in the UK general population.Findings
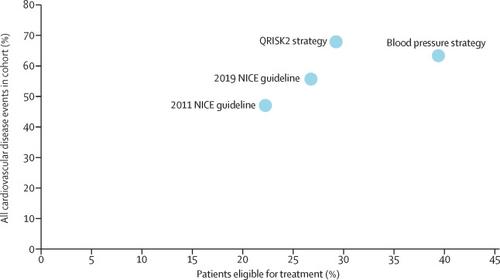
Between Jan 1, 2011, and March 31, 2016, 1 222 670 patients in the cohort were followed up for a median of 4·3 years (IQR 2·5–5·2). 271 963 (22·2%) patients were eligible for treatment under the 2011 NICE guideline, 327 429 (26·8%) under the proposed 2019 NICE guideline, 481 859 (39·4%) on the basis of a blood pressure threshold of 140/90 mm Hg or higher, and 357 840 (29·3%) on the basis of a QRISK2 threshold of 10% or higher. During follow-up, 32 183 patients were diagnosed with cardiovascular disease (overall rate 7·1 per 1000 person-years, 95% CI 7·0–7·2). Cardiovascular event rates in patients eligible for each strategy were 15·2 per 1000 person-years (95% CI 15·0–15·5) under the 2011 NICE guideline, 14·9 (14·7–15·1) under the proposed 2019 NICE guideline, 11·4 (11·3–11·6) with blood pressure threshold alone, and 16·9 (16·7–17·1) with QRISK2 threshold alone. Scaled to the UK population, we estimated that 233 152 events would be avoided under the 2011 NICE guideline (28 patients needed to treat for 10 years to avoid one event), 270 233 under the 2019 NICE guideline (29 patients), 301 523 using a blood pressure threshold (38 patients), and 322 921 using QRISK2 threshold (27 patients).Interpretation
A cardiovascular risk-based strategy (QRISK2 ≥10%) could prevent over a third more cardiovascular disease events than the 2011 NICE guideline and a fifth more than the 2019 NICE guideline, with similar efficiency regarding number treated per event avoided.Funding
National Institute for Health Research.中文翻译:
四种降压治疗策略的资格和随后的心血管疾病负担:一项回顾性队列研究
背景
尽管有强有力的证据表明,在整个血压范围内的患者中都观察到了降低血压的益处,但全球范围内降低血压的治疗建议仍然主要以血压阈值为指导。在这项研究中,我们旨在以英国为例,调查提供血压治疗的替代策略的影响。
方法
我们对 30-79 岁无心血管疾病的初级保健患者进行了一项回顾性队列研究,使用的数据来自与医院发病统计和国家统计局死亡率相关的英国临床实践研究数据链。我们评估和比较了四种不同的策略来确定治疗资格:使用 2011 年英国国家健康与护理卓越研究所 (NICE) 指南,或提议的 2019 年 NICE 指南,或单独血压(阈值≥140/90 mm Hg),或预测仅 10 年心血管风险(QRISK2 评分≥10%)。对患者进行随访,直至最早发生心血管疾病诊断、死亡或随访期结束(2016 年 3 月 31 日)。对于每种策略,我们估计了符合治疗条件的患者比例以及可以通过治疗预防的心血管事件的数量。然后,我们估计了英国普通人群的资格和 10 年内将发生的事件数量。
发现
2011年1月1日至2016年3月31日期间,队列中的1 222 670名患者接受了中位随访4·3年(IQR 2·5–5·2)。根据 2011 年 NICE 指南,有 271 963 名患者 (22·2%) 有资格接受治疗;根据 2019 年 NICE 指南,有 327 429 名患者 (26·8%) 符合治疗资格;根据血压阈值,有 481 859 名患者 (39·4%) 有资格接受治疗140/90 mm Hg 或更高,以及 357 840 (29·3%)(基于 10% 或更高的 QRISK2 阈值)。随访期间,32 183 名患者被诊断患有心血管疾病(总体发病率为每 1000 人年 7·1,95% CI 7·0–7·2)。根据 2011 年 NICE 指南,符合每种策略的患者的心血管事件发生率为每 1000 人年 15·2 例(95% CI 15·0–15·5),根据 2011 年 NICE 指南,每 1000 人年为 14·9(14·7–15·1)。提出的 2019 年 NICE 指南,11·4 (11·3–11·6) 仅包含血压阈值,16·9 (16·7–17·1) 仅包含 QRISK2 阈值。根据英国人口规模,我们估计根据 2011 年 NICE 指南可以避免 233 152 起事件(28 名患者需要治疗 10 年才能避免一件事件),根据 2019 年 NICE 指南(29 名患者)可以避免 270 233 起事件,使用 2019 年 NICE 指南可以避免 301 523 起事件。血压阈值(38 名患者),以及 322 921 使用 QRISK2 阈值(27 名患者)。
解释
基于心血管风险的策略(QRISK2≥10%)可以比 2011 年 NICE 指南多预防三分之一以上的心血管疾病事件,比 2019 年 NICE 指南多五分之一,并且在每次避免事件的治疗数量方面具有相似的效率。
资金
国家健康研究所。










































 京公网安备 11010802027423号
京公网安备 11010802027423号