当前位置:
X-MOL 学术
›
Prostate Cancer Prostatic. Dis.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Analysis of the prognostic utility of the cell cycle progression (CCP) score generated from needle biopsy in men treated with definitive therapy.
Prostate Cancer and Prostatic Diseases ( IF 5.1 ) Pub Date : 2019-06-27 , DOI: 10.1038/s41391-019-0159-9 Daniel J Canter 1, 2 , Stephen Freedland 3 , Saradha Rajamani 4 , Maria Latsis 1 , Margaret Variano 1 , Shams Halat 1 , Jonathan Tward 5 , Todd Cohen 4 , Steven Stone 4 , Thorsten Schlomm 6 , Jay Bishoff 7 , Stephen Bardot 1, 2
Prostate Cancer and Prostatic Diseases ( IF 5.1 ) Pub Date : 2019-06-27 , DOI: 10.1038/s41391-019-0159-9 Daniel J Canter 1, 2 , Stephen Freedland 3 , Saradha Rajamani 4 , Maria Latsis 1 , Margaret Variano 1 , Shams Halat 1 , Jonathan Tward 5 , Todd Cohen 4 , Steven Stone 4 , Thorsten Schlomm 6 , Jay Bishoff 7 , Stephen Bardot 1, 2
Affiliation
|
BACKGROUND
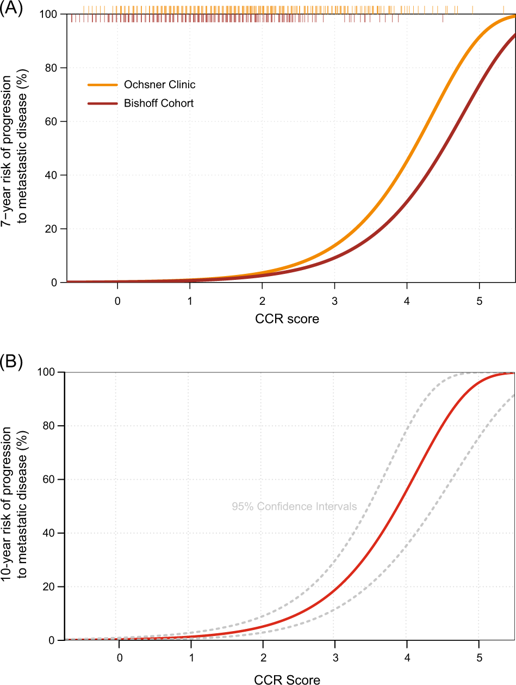
Accurate risk stratification can help guide appropriate treatment decisions in men with localized prostate cancer. Here, we evaluated the independent ability of the molecular cell cycle progression (CCP) score and the combined cell-cycle clinical risk (CCR) score to predict 10-year risk of progression to metastatic disease in a large, pooled analysis of men with definitively treated prostate cancer.
METHODS
The pooled analysis included 1,062 patients from four institutions (Martini Clinic, Durham VA Medical Center, Intermountain Healthcare, Ochsner Clinic) treated definitively for localized prostate cancer by either radical prostatectomy or radiotherapy (brachytherapy or external beam radiotherapy ± hormone therapy). The CCP score was determined using the RNA expression of 46 genes from archival formalin-fixed paraffin-embedded biopsy tissue. The CCR score was calculated using a predefined linear combination of the CCP score and the Cancer of the Prostate Risk Assessment (CAPRA) score. The scores were evaluated for association with 10-year risk of metastatic disease following definitive therapy after adjusting for other clinical variables.
RESULTS
The CCP score was strongly associated with 10-year risk of metastatic disease in multivariable analysis [Hazard Ratio per unit score = 2.21; 95% confidence interval (CI) 1.64, 2.98; p = 1.9 × 10-6] after adjusting for CAPRA, treatment type, and cohort. CCR was also highly prognostic (Hazard Ratio per unit score = 4.00; 95% CI 2.95, 5.42; p = 6.3 × 10-21). There was no evidence of interaction between CCP or CCR and cohort (p = 0.79 and p = 0.86, respectively) or treatment type (p = 0.55 and p = 0.78, respectively). Observed patient CCR-based predicted risks for metastatic disease by 10 years ranged from 0.1 to 99.4%, (IQR 0.7%, 4.6%).
CONCLUSIONS
Both CCP and CCR scores provided independent prognostic information for predicting progression to metastatic disease after both surgery and radiation. These results further demonstrate their potential use as a risk stratification tool in patients with newly-diagnosed prostate cancer.
中文翻译:

对接受最终疗法治疗的男性进行穿刺活检得出的细胞周期进展(CCP)评分对预后的效用进行分析。
背景技术准确的风险分层可以帮助指导局部前列腺癌男性的适当治疗决策。在这里,我们通过对确定性男性的大型汇总分析,评估了分子细胞周期进展(CCP)评分和细胞周期临床风险综合(CCR)评分的独立能力,以预测10年发展为转移性疾病的风险。治疗前列腺癌。方法汇总分析包括来自四个机构(马提尼诊所,达勒姆VA医疗中心,山间医疗保健,奥克斯纳诊所)的1,062例患者,这些患者通过根治性前列腺切除术或放射疗法(近距离放射疗法或外照射放射疗法±激素疗法)明确治疗了局部前列腺癌。使用来自福尔马林档案固定石蜡包埋的活检组织的46个基因的RNA表达来确定CCP评分。使用CCP评分和前列腺癌风险评估(CAPRA)评分的预定义线性组合来计算CCR评分。调整其他临床变量后,评估分数与确定治疗后10年转移性疾病风险的相关性。结果在多变量分析中,CCP评分与10年转移性疾病的风险密切相关[每单位评分的危险比= 2.21;95%置信区间(CI)1.64,2.98; p = 1.9×10-6]在调整了CAPRA,治疗类型和队列后。CCR也具有较高的预后性(每单位评分的危险比= 4.00; 95%CI 2.95,5.42; p = 6.3×10-21)。没有证据表明CCP或CCR与队列(分别为p = 0.79和p = 0.86)或治疗类型(分别为p = 0.55和p = 0.78)之间存在相互作用。观察到的基于患者CCR的10年转移性疾病的预测风险范围为0.1%至99.4%(IQR 0.7%,4.6%)。结论CCP和CCR评分均提供了独立的预后信息,可用于预测手术和放疗后转移性疾病的进展。这些结果进一步证明了它们在新诊断的前列腺癌患者中作为危险分层工具的潜在用途。结论CCP和CCR评分均提供了独立的预后信息,可用于预测手术和放疗后转移性疾病的进展。这些结果进一步证明了它们在新诊断的前列腺癌患者中作为危险分层工具的潜在用途。结论CCP和CCR评分均提供了独立的预后信息,可用于预测手术和放疗后转移性疾病的进展。这些结果进一步证明了它们在新诊断的前列腺癌患者中作为危险分层工具的潜在用途。
更新日期:2019-11-18
中文翻译:
对接受最终疗法治疗的男性进行穿刺活检得出的细胞周期进展(CCP)评分对预后的效用进行分析。
背景技术准确的风险分层可以帮助指导局部前列腺癌男性的适当治疗决策。在这里,我们通过对确定性男性的大型汇总分析,评估了分子细胞周期进展(CCP)评分和细胞周期临床风险综合(CCR)评分的独立能力,以预测10年发展为转移性疾病的风险。治疗前列腺癌。方法汇总分析包括来自四个机构(马提尼诊所,达勒姆VA医疗中心,山间医疗保健,奥克斯纳诊所)的1,062例患者,这些患者通过根治性前列腺切除术或放射疗法(近距离放射疗法或外照射放射疗法±激素疗法)明确治疗了局部前列腺癌。使用来自福尔马林档案固定石蜡包埋的活检组织的46个基因的RNA表达来确定CCP评分。使用CCP评分和前列腺癌风险评估(CAPRA)评分的预定义线性组合来计算CCR评分。调整其他临床变量后,评估分数与确定治疗后10年转移性疾病风险的相关性。结果在多变量分析中,CCP评分与10年转移性疾病的风险密切相关[每单位评分的危险比= 2.21;95%置信区间(CI)1.64,2.98; p = 1.9×10-6]在调整了CAPRA,治疗类型和队列后。CCR也具有较高的预后性(每单位评分的危险比= 4.00; 95%CI 2.95,5.42; p = 6.3×10-21)。没有证据表明CCP或CCR与队列(分别为p = 0.79和p = 0.86)或治疗类型(分别为p = 0.55和p = 0.78)之间存在相互作用。观察到的基于患者CCR的10年转移性疾病的预测风险范围为0.1%至99.4%(IQR 0.7%,4.6%)。结论CCP和CCR评分均提供了独立的预后信息,可用于预测手术和放疗后转移性疾病的进展。这些结果进一步证明了它们在新诊断的前列腺癌患者中作为危险分层工具的潜在用途。结论CCP和CCR评分均提供了独立的预后信息,可用于预测手术和放疗后转移性疾病的进展。这些结果进一步证明了它们在新诊断的前列腺癌患者中作为危险分层工具的潜在用途。结论CCP和CCR评分均提供了独立的预后信息,可用于预测手术和放疗后转移性疾病的进展。这些结果进一步证明了它们在新诊断的前列腺癌患者中作为危险分层工具的潜在用途。








































 京公网安备 11010802027423号
京公网安备 11010802027423号