当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Standardized Team-Based Care for Cardiogenic Shock
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-04-01 , DOI: 10.1016/j.jacc.2018.12.084 Behnam N Tehrani 1 , Alexander G Truesdell 2 , Matthew W Sherwood 1 , Shashank Desai 1 , Henry A Tran 1 , Kelly C Epps 1 , Ramesh Singh 1 , Mitchell Psotka 1 , Palak Shah 1 , Lauren B Cooper 1 , Carolyn Rosner 1 , Anika Raja 1 , Scott D Barnett 1 , Patricia Saulino 1 , Christopher R deFilippi 1 , Paul A Gurbel 1 , Charles E Murphy 1 , Christopher M O'Connor 1
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-04-01 , DOI: 10.1016/j.jacc.2018.12.084 Behnam N Tehrani 1 , Alexander G Truesdell 2 , Matthew W Sherwood 1 , Shashank Desai 1 , Henry A Tran 1 , Kelly C Epps 1 , Ramesh Singh 1 , Mitchell Psotka 1 , Palak Shah 1 , Lauren B Cooper 1 , Carolyn Rosner 1 , Anika Raja 1 , Scott D Barnett 1 , Patricia Saulino 1 , Christopher R deFilippi 1 , Paul A Gurbel 1 , Charles E Murphy 1 , Christopher M O'Connor 1
Affiliation
|
BACKGROUND
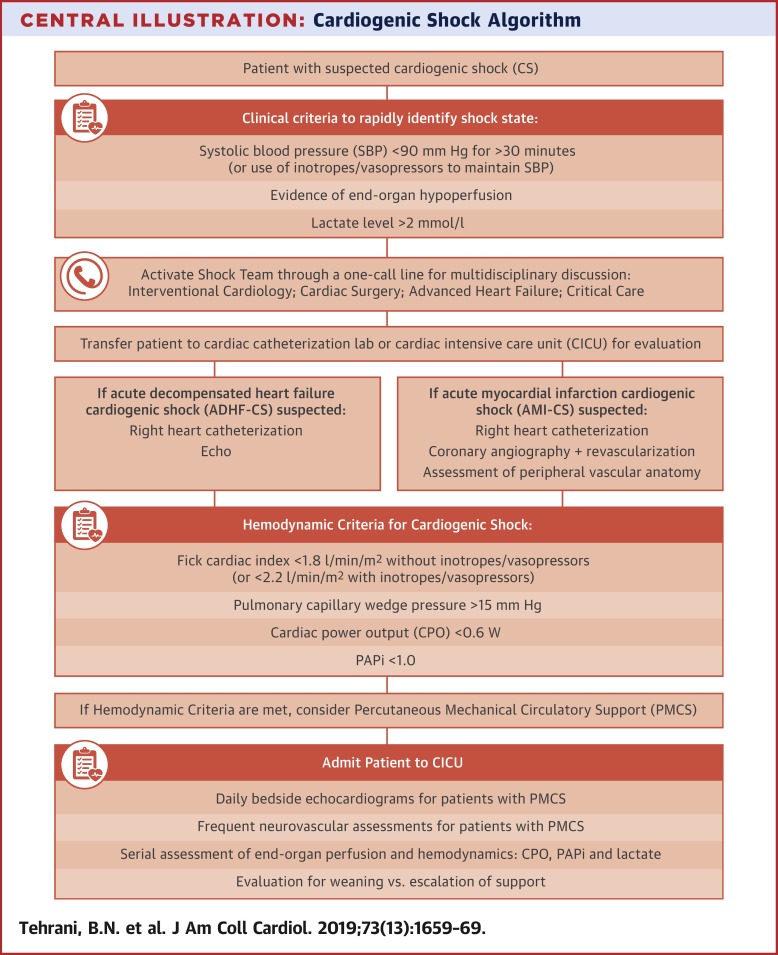
Cardiogenic shock (CS) is a multifactorial, hemodynamically complex syndrome associated with high mortality. Despite advances in reperfusion and mechanical circulatory support, management remains highly variable and outcomes poor. OBJECTIVES
This study investigated whether a standardized team-based approach can improve outcomes in CS and whether a risk score can guide clinical decision making. METHODS
A total of 204 consecutive patients with CS were identified. CS etiology, patient demographic characteristics, right heart catheterization, mechanical circulatory support use, and survival were determined. Cardiac power output (CPO) and pulmonary arterial pulsatility index (PAPi) were measured at baseline and 24 h after the CS diagnosis. Thresholds at 24 h for lactate (<3.0 mg/dl), CPO (>0.6 W), and PAPi (>1.0) were determined. Using logistic regression analysis, a validated risk stratification score was developed. RESULTS
Compared with 30-day survival of 47% in 2016, 30-day survival in 2017 and 2018 increased to 57.9% and 76.6%, respectively (p < 0.01). Independent predictors of 30-day mortality were age ≥71 years, diabetes mellitus, dialysis, ≥36 h of vasopressor use at time of diagnosis, lactate levels ≥3.0 mg/dl, CPO <0.6 W, and PAPi <1.0 at 24 h after diagnosis and implementation of therapies. Either 1 or 2 points were assigned to each variable, and a 3-category risk score was determined: 0 to 1 (low), 2 to 4 (moderate), and ≥5 (high). CONCLUSIONS
This observational study suggests that a standardized team-based approach may improve CS outcomes. A score incorporating demographic, laboratory, and hemodynamic data may be used to quantify risk and guide clinical decision-making for all phenotypes of CS.
中文翻译:

心源性休克的标准化团队护理
背景心源性休克 (CS) 是一种多因素、血流动力学复杂的综合征,与高死亡率相关。尽管在再灌注和机械循环支持方面取得了进展,但管理仍然高度可变且结果不佳。目标 本研究调查了基于团队的标准化方法是否可以改善 CS 的结果,以及风险评分是否可以指导临床决策。方法共确定了 204 名连续的 CS 患者。确定了 CS 病因、患者人口统计学特征、右心导管插入术、机械循环支持的使用和存活率。在基线和 CS 诊断后 24 小时测量心脏功率输出 (CPO) 和肺动脉搏动指数 (PAPi)。确定了乳酸 (<3.0 mg/dl)、CPO (>0.6 W) 和 PAPi (>1.0) 的 24 小时阈值。使用逻辑回归分析,开发了经过验证的风险分层评分。结果 与 2016 年 47% 的 30 天生存率相比,2017 年和 2018 年的 30 天生存率分别提高到 57.9% 和 76.6%(p < 0.01)。30 天死亡率的独立预测因素是年龄≥71 岁、糖尿病、透析、诊断时使用血管加压药≥36 小时、乳酸水平≥3.0 mg/dl、CPO <0.6 W 和 PAPi <1.0 在 24 小时后诊断和治疗的实施。为每个变量分配 1 或 2 分,并确定 3 类风险评分:0 到 1(低)、2 到 4(中)和≥5(高)。结论 这项观察性研究表明,标准化的基于团队的方法可能会改善 CS 结果。综合人口统计、实验室、
更新日期:2019-04-01
中文翻译:
心源性休克的标准化团队护理
背景心源性休克 (CS) 是一种多因素、血流动力学复杂的综合征,与高死亡率相关。尽管在再灌注和机械循环支持方面取得了进展,但管理仍然高度可变且结果不佳。目标 本研究调查了基于团队的标准化方法是否可以改善 CS 的结果,以及风险评分是否可以指导临床决策。方法共确定了 204 名连续的 CS 患者。确定了 CS 病因、患者人口统计学特征、右心导管插入术、机械循环支持的使用和存活率。在基线和 CS 诊断后 24 小时测量心脏功率输出 (CPO) 和肺动脉搏动指数 (PAPi)。确定了乳酸 (<3.0 mg/dl)、CPO (>0.6 W) 和 PAPi (>1.0) 的 24 小时阈值。使用逻辑回归分析,开发了经过验证的风险分层评分。结果 与 2016 年 47% 的 30 天生存率相比,2017 年和 2018 年的 30 天生存率分别提高到 57.9% 和 76.6%(p < 0.01)。30 天死亡率的独立预测因素是年龄≥71 岁、糖尿病、透析、诊断时使用血管加压药≥36 小时、乳酸水平≥3.0 mg/dl、CPO <0.6 W 和 PAPi <1.0 在 24 小时后诊断和治疗的实施。为每个变量分配 1 或 2 分,并确定 3 类风险评分:0 到 1(低)、2 到 4(中)和≥5(高)。结论 这项观察性研究表明,标准化的基于团队的方法可能会改善 CS 结果。综合人口统计、实验室、










































 京公网安备 11010802027423号
京公网安备 11010802027423号