Drugs & Aging ( IF 2.8 ) Pub Date : 2024-03-11 , DOI: 10.1007/s40266-024-01103-2 Ashna Talwar , Satabdi Chatterjee , Jeffrey Sherer , Susan Abughosh , Michael Johnson , Rajender R. Aparasu
|
Background
Cumulative anticholinergic burden refers to the cumulative effect of multiple medications with anticholinergic properties. However, concomitant use of cholinesterase inhibitors (ChEIs) and anticholinergic burden can nullify the benefit of the treatment and worsen Alzheimer’s disease (AD). A literature gap exists regarding the extent of the cumulative anticholinergic burden and associated risk factors in AD. Therefore, this study evaluated the prevalence and predictors of cumulative anticholinergic burden among patients with AD initiating ChEIs.
Methods
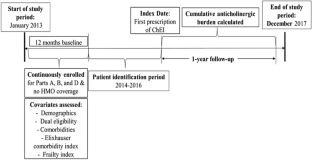
A retrospective longitudinal cohort study was conducted using the Medicare claims data involving parts A, B, and D from 2013 to 2017. The study sample included older adults (65 years and older) diagnosed with AD and initiating ChEIs (donepezil, rivastigmine, or galantamine). The cumulative anticholinergic burden was calculated based on the Anticholinergic Cognitive Burden scale and patient-specific dosing using the defined daily dose over the 1 year follow-up period after ChEI initiation. Incremental anticholinergic burden levels were dichotomized into moderate–high (sum of standardized daily anticholinergic exposure over a year (TSDD) score ≥ 90) versus low–no (score 0–89). The Andersen Behavioral Model was used as the conceptual framework for selecting the predictors under the predisposing, enabling, and need categories. A multivariable logistic regression model was used to evaluate the predictors of high-moderate versus low–no cumulative anticholinergic burden. A multinomial logistic regression model was also used to determine the factors associated with patients having moderate and high burdens compared to low/no burdens.
Results
The study included 222,064 older adults with AD with incident ChEI use (mean age 82.24 ± 7.29, 68.9% females, 83.6% White). Overall, 80.48% had some anticholinergic burden during the follow-up, with 36.26% patients with moderate (TSDD scores 90–499), followed by 24.76% high (TSDD score > 500), and 19.46% with low (TSDD score 1–89) burden categories. Predisposing factors such as age; African American, Asian, or Hispanic race; and need factors included comorbidities such as dyslipidemia, syncope, delirium, fracture, pneumonia, epilepsy, and claims-based frailty index were less likely to be associated with the moderate–high anticholinergic burden. The factors that increased the odds of moderate–high burden were predisposing factors such as female sex; enabling factors such as dual eligibility and diagnosis year; and need factors such as baseline burden, behavioral and psychological symptoms of dementia, depression, insomnia, urinary incontinence, irritable bowel syndrome, anxiety, muscle spasm, gastroesophageal reflux disease, heart failure, and dysrhythmia. Most of these findings remained consistent with multinomial logistic regression.
Conclusion
Four out of five older adults with AD had some level of anticholinergic burden, with over 60% having moderate–high anticholinergic burden. Several predisposing, enabling, and need factors were associated with the cumulative anticholinergic burden. The study findings suggest a critical need to minimize the cumulative anticholinergic burden to improve AD care.
中文翻译:
患有阿尔茨海默病的老年人的累积抗胆碱能负担及其预测因素启动胆碱酯酶抑制剂
背景
累积抗胆碱能负荷是指多种具有抗胆碱能特性的药物的累积效应。然而,同时使用胆碱酯酶抑制剂 (ChEI) 和抗胆碱能药物可能会抵消治疗效果,并使阿尔茨海默病 (AD) 恶化。关于 AD 中累积抗胆碱能负荷的程度和相关危险因素,存在文献空白。因此,本研究评估了启动 ChEI 的 AD 患者中累积抗胆碱能负荷的患病率和预测因素。
方法
使用 2013 年至 2017 年涉及 A、B 和 D 部分的医疗保险索赔数据进行了一项回顾性纵向队列研究。研究样本包括诊断为 AD 并开始使用 ChEI(多奈哌齐、卡巴拉汀或加兰他敏)的老年人(65 岁及以上) )。累积抗胆碱能负担是根据抗胆碱能认知负担量表和患者特定剂量计算的,使用 ChEI 启动后 1 年随访期内规定的每日剂量。增量抗胆碱能负荷水平分为中-高(一年内标准化每日抗胆碱能暴露总和(TSDD)评分≥ 90)与低-无(评分0-89)。安徒生行为模型被用作在倾向、促成和需求类别下选择预测变量的概念框架。使用多变量逻辑回归模型来评估高-中度与低-无累积抗胆碱能负荷的预测因子。还使用多项逻辑回归模型来确定与低/无负担患者相比,中度和高负担患者的相关因素。
结果
该研究纳入了 222,064 名患有 AD 且偶然使用 ChEI 的老年人(平均年龄 82.24 ± 7.29,其中 68.9% 为女性,83.6% 为白人)。总体而言,80.48% 的患者在随访期间有一定的抗胆碱能负担,其中 36.26% 的患者为中度(TSDD 评分 90-499),其次是 24.76% 高(TSDD 评分 > 500),19.46% 为低(TSDD 评分 1-4)。 89)负担类别。年龄等诱发因素;非裔美国人、亚洲人或西班牙人种;需求因素包括血脂异常、晕厥、谵妄、骨折、肺炎、癫痫等合并症,以及基于索赔的虚弱指数与中高抗胆碱能负担相关的可能性较小。增加中高负担几率的因素是女性性别等诱发因素;双重资格和诊断年份等促成因素;以及需要因素,例如基线负担、痴呆、抑郁、失眠、尿失禁、肠易激综合征、焦虑、肌肉痉挛、胃食管反流病、心力衰竭和心律失常的行为和心理症状。大多数这些发现与多项逻辑回归保持一致。
结论
五分之四的患有 AD 的老年人有一定程度的抗胆碱能负担,其中超过 60% 的人有中度至高抗胆碱能负担。一些诱发因素、促成因素和需求因素与累积的抗胆碱能负担有关。研究结果表明,迫切需要最大限度地减少累积的抗胆碱能负担,以改善 AD 护理。


























 京公网安备 11010802027423号
京公网安备 11010802027423号