The Indian Journal of Pediatrics ( IF 4.3 ) Pub Date : 2023-12-29 , DOI: 10.1007/s12098-023-04925-x Lalit Takia , Arun K. Baranwal , Pramod K. Gupta , Muralidharan Jayashree , Suresh Kumar Angurana
|
Objectives
To assess the efficacy and safety of bicarbonate infusion in children with Acute Diarrhea and Severe Dehydration (ADSD) having severe Non-Anion Gap Metabolic Acidemia (sNAGMA).
Methods
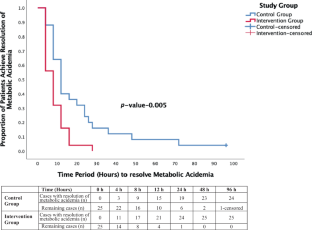
Children (aged 1–144 mo) with ADSD and sNAGMA (pH ≤7.2 and/or serum bicarbonate ≤15 mEq/L) were enrolled in an open-label randomized design. Controls (n = 25) received WHO-recommended rehydration therapy with Ringer Lactate, while intervention group (n = 25) received additional bicarbonate deficit correction. Primary outcome was time taken to resolve metabolic acidemia (pH >7.30 and/or bicarbonate >15 mEq/L). Secondary outcome measures were adverse outcome [composite of pediatric intensive care unit (PICU) transfer and deaths], acute care area free days in 5 d (ACAFD5), hospital stay, and adverse effects.
Results
Time taken to resolve metabolic acidemia was significantly lesser with intervention [median (IQR); 8 h (4, 12) vs. 12 h (8, 24); p = 0.0067]. Intervention led to acidemia resolution in significantly more children by 8 h and 16 h (17/25 vs. 9/25, p = 0.035 and 23/25 vs. 17/24, p = 0.018, respectively). Patients with fluid refractory shock needed lesser inotropes in intervention group [median Vasoactive Inotrope Score (VIS), 10.5 vs. 34]. Intervention led to significantly lesser adverse outcome (0/25 vs. 5/25, p = 0.049), and noticeably more ACAFD5 [median (IQR); 2 (1, 2) vs. 1 (1, 2); p = 0.12]. Two patients died in the control group while none in the intervention group. No adverse effect was documented.
Conclusions
Additional calculated dose of bicarbonate infusion led to significantly early resolution of metabolic acidemia, lesser utilization of critical care facilities, and lesser adverse outcome in children with ADSD and sNAGMA, compared to standard therapy, with no adverse effect.
中文翻译:
额外碳酸氢盐输注补充世界卫生组织补液疗法治疗患有急性腹泻和严重脱水并伴有严重非阴离子间隙代谢性酸血症的儿童:一项开放标签随机试验
目标
评估碳酸氢盐输注对患有严重非阴离子间隙代谢性酸血症 (sNAGMA) 的急性腹泻和严重脱水 (ADSD) 儿童的疗效和安全性。
方法
患有 ADSD 和 sNAGMA(pH ≤ 7.2 和/或血清碳酸氢盐 ≤ 15 mEq/L)的儿童(1-144 个月)被纳入开放标签随机设计。对照组(n = 25)接受世界卫生组织推荐的乳酸林格氏补液疗法,而干预组(n = 25)接受额外的碳酸氢盐缺乏校正。主要结局是解决代谢性酸血症(pH > 7.30 和/或碳酸氢盐 > 15 mEq/L)所需的时间。次要结局指标是不良结局[儿科重症监护病房 (PICU) 转移和死亡的综合情况]、5 天内的急性护理区空闲天数 (ACAFD 5 )、住院时间和不良反应。
结果
通过干预,解决代谢性酸血症所需的时间显着缩短[中位数(IQR);8 小时(4、12)与 12 小时(8、24);p = 0.0067]。干预使更多儿童在 8 小时和 16 小时内酸血症得到缓解(分别为 17/25 与 9/25,p = 0.035 和 23/25 与 17/24,p = 0.018)。液体难治性休克患者在干预组中需要较少的正性肌力药物[中位血管活性正性肌力评分 (VIS),10.5 比 34]。干预导致不良结果显着减少(0/25 vs. 5/25,p = 0.049),并且 ACAFD 5 [中位数(IQR);2 (1, 2) 与 1 (1, 2);p = 0.12]。对照组有两名患者死亡,而干预组没有一名患者死亡。没有记录到不良反应。
结论
与标准治疗相比,额外计算剂量的碳酸氢盐输注可显着提早解决代谢性酸血症,减少重症监护设施的使用,并减少 ADSD 和 sNAGMA 儿童的不良后果,且无不良反应。


























 京公网安备 11010802027423号
京公网安备 11010802027423号