EPMA Journal ( IF 6.5 ) Pub Date : 2023-11-15 , DOI: 10.1007/s13167-023-00341-5 Simon M. Frey , Adam Bakula , Andrew Tsirkin , Vasily Vasilchenko , Peter Ruff , Caroline Oehri , Melissa Fee Amrein , Gabrielle Huré , Klara Rumora , Ibrahim Schäfer , Federico Caobelli , Philip Haaf , Christian E. Mueller , Bjoern Andrew Remppis , Hans-Peter Brunner-La Rocca , Michael J. Zellweger
|
Background
Patients are referred to functional coronary artery disease (CAD) testing based on their pre-test probability (PTP) to search for myocardial ischemia. The recommended prediction tools incorporate three variables (symptoms, age, sex) and are easy to use, but have a limited diagnostic accuracy. Hence, a substantial proportion of non-invasive functional tests reveal no myocardial ischemia, leading to unnecessary radiation exposure and costs. Therefore, preselection of patients before ischemia testing needs to be improved using a more predictive and personalised approach.
Aims
Using multiple variables (symptoms, vitals, ECG, biomarkers), artificial intelligence–based tools can provide a detailed and individualised profile of each patient. This could improve PTP assessment and provide a more personalised diagnostic approach in the framework of predictive, preventive and personalised medicine (PPPM).
Methods
Consecutive patients (n = 2417) referred for Rubidium-82 positron emission tomography were evaluated. PTP was calculated using the ESC 2013/2019 and ACC 2012/2021 guidelines, and a memetic pattern–based algorithm (MPA) was applied incorporating symptoms, vitals, ECG and biomarkers. Five PTP categories from very low to very high PTP were defined (i.e., < 5%, 5–15%, 15–50%, 50–85%, > 85%). Ischemia was defined as summed difference score (SDS) ≥ 2.
Results
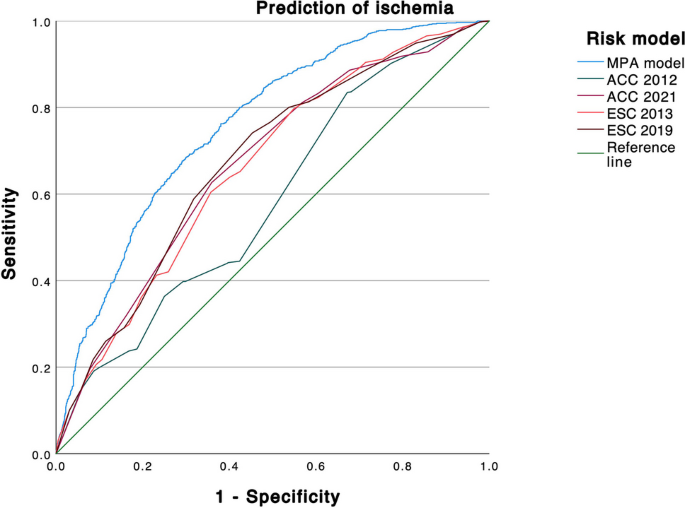
Ischemia was present in 37.1%. The MPA model was most accurate to predict ischemia (AUC: 0.758, p < 0.001 compared to ESC 2013, 0.661; ESC 2019, 0.673; ACC 2012, 0.585; ACC 2021, 0.667). Using the < 5% threshold, the MPA’s sensitivity and negative predictive value to rule out ischemia were 99.1% and 96.4%, respectively. The model allocated patients more evenly across PTP categories, reduced the proportion of patients in the intermediate (15–85%) range by 29% (ACC 2012)–51% (ESC 2019), and was the only tool to correctly predict ischemia prevalence in the very low PTP category.
Conclusion
The MPA model enhanced ischemia testing according to the PPPM framework:
-
1)
The MPA model improved individual prediction of ischemia significantly and could safely exclude ischemia based on readily available variables without advanced testing (“predictive”).
-
2)
It reduced the proportion of patients in the intermediate PTP range. Therefore, it could be used as a gatekeeper to prevent patients from further unnecessary downstream testing, radiation exposure and costs (“preventive”).
-
3)
Consequently, the MPA model could transform ischemia testing towards a more personalised diagnostic algorithm (“personalised”).
中文翻译:
人工智能改善铷正电子发射断层扫描中的缺血预测——一项验证研究
背景
根据患者的预测试概率 (PTP),将患者转介至功能性冠状动脉疾病 (CAD) 测试,以寻找心肌缺血。推荐的预测工具包含三个变量(症状、年龄、性别),易于使用,但诊断准确性有限。因此,相当一部分非侵入性功能测试未发现心肌缺血,从而导致不必要的辐射暴露和费用。因此,需要使用更具预测性和个性化的方法来改进缺血测试前的患者预选。
目标
使用多个变量(症状、生命体征、心电图、生物标志物),基于人工智能的工具可以提供每位患者的详细且个性化的概况。这可以改善 PTP 评估,并在预测、预防和个性化医学 (PPPM) 框架内提供更加个性化的诊断方法。
方法
对转诊接受铷-82 正电子发射断层扫描的连续患者 ( n = 2417) 进行了评估。PTP 使用 ESC 2013/2019 和 ACC 2012/2021 指南计算,并应用基于模因模式的算法 (MPA),结合症状、生命体征、心电图和生物标志物。定义了从极低到极高 PTP 的五个 PTP 类别(即 < 5%、5–15%、15–50%、50–85%、> 85%)。缺血定义为总差评分 (SDS) ≥ 2。
结果
37.1% 存在缺血。MPA 模型预测缺血最准确(AUC:0.758, 与 ESC 2013,0.661 相比,p < 0.001;ESC 2019,0.673;ACC 2012,0.585;ACC 2021,0.667)。使用 < 5% 阈值,MPA 排除缺血的敏感性和阴性预测值分别为 99.1% 和 96.4%。该模型在 PTP 类别中更均匀地分配患者,将中间 (15-85%) 范围内的患者比例减少 29% (ACC 2012)–51% (ESC 2019),并且是正确预测缺血发生率的唯一工具属于非常低的 PTP 类别。
结论
MPA模型根据PPPM框架增强了缺血测试:
-
1)
MPA 模型显着改善了个体对缺血的预测,并且可以根据现成的变量安全地排除缺血,而无需进行高级测试(“预测”)。
-
2)
它减少了处于中间 PTP 范围的患者比例。因此,它可以用作看门人,防止患者进行进一步不必要的下游测试、辐射暴露和费用(“预防性”)。
-
3)
因此,MPA 模型可以将缺血测试转变为更加个性化的诊断算法(“个性化”)。


























 京公网安备 11010802027423号
京公网安备 11010802027423号