Journal of Hepatology ( IF 26.8 ) Pub Date : 2023-04-21 , DOI: 10.1016/j.jhep.2023.04.002 Maria Kjaergaard 1 , Katrine Prier Lindvig 1 , Katrine Holtz Thorhauge 1 , Peter Andersen 2 , Johanne Kragh Hansen 1 , Nanna Kastrup 3 , Jane Møller Jensen 2 , Camilla Dalby Hansen 1 , Stine Johansen 1 , Mads Israelsen 2 , Nikolaj Torp 1 , Morten Beck Trelle 4 , Shan Shan 5 , Sönke Detlefsen 6 , Steen Antonsen 7 , Jørgen Ellegaard Andersen 8 , Isabel Graupera 9 , Pere Ginés 9 , Maja Thiele 1 , Aleksander Krag 10
|
Background & Aims
There is a need for accurate biomarkers of fibrosis for population screening of alcohol-related and non-alcoholic fatty liver disease (ALD, NAFLD). We compared the performance of the enhanced liver fibrosis (ELF) test to the fibrosis-4 index (FIB-4) and NAFLD fibrosis score (NFS), using transient elastography as the reference standard.
Methods
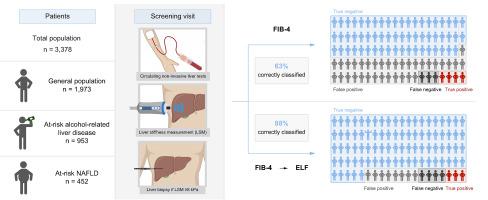
We prospectively included participants from the general population, and people at risk of ALD or NAFLD. Screening positive participants (TE ≥8 kPa) were offered a liver biopsy. We measured concomitant ELF, FIB-4, and NFS using validated cut-offs: ≥9.8, ≥1.3, ≥-1.45, respectively.
Results
We included 3,378 participants (1,973 general population, 953 at risk of ALD, 452 at risk of NAFLD), with a median age of 57 years (IQR: 51-63). Two hundred-and-forty-two were screening positive (3.4% in the general population, 12%/14% who were at-risk of ALD/NAFLD, respectively). Most participants with TE <8 kPa also had ELF <9.8 (88%) despite a poor overall correlation between ELF and TE (Spearman´s rho = 0.207). ELF was associated with significantly fewer false positives (11%) than FIB-4 and NFS (35% and 45%), while retaining a low rate of false negatives (<8%). A screening strategy of FIB-4 followed by ELF in indeterminate cases resulted in false positives in 8%, false negatives in 4% and the correct classification in 88% of cases. We performed a liver biopsy in 155/242 (64%) patients who screened positive, of whom 54 (35%) had advanced fibrosis (≥F3). ELF diagnosed advanced fibrosis with significantly better diagnostic accuracy than FIB-4 and NFS: AUROC 0.85 (95% CI 0.79-0.92) vs. 0.73 (0.64-0.81) and 0.66 (0.57-0.76), respectively.
Conclusion
The ELF test alone or combined with FIB-4 for liver fibrosis screening in the general population and at-risk groups reduces the number of futile referrals compared to FIB-4 and NFS, without overlooking true cases.
Impact and implications
We need referral pathways that are efficient at detecting advanced fibrosis from alcohol-related and non-alcoholic fatty liver disease in the population, but without causing futile referrals or excessive use of resources. This study indicates that a sequential test strategy of FIB-4 followed by the ELF test in indeterminate cases leads to few patients referred for confirmatory liver stiffness measurement, while retaining a high rate of detected cases, and at low direct costs. This two-step referral pathway could be used by primary care for mass, targeted, or opportunistic screening for liver fibrosis in the population.
Clinical trial number
Clinicaltrials.gov number NCT03308916.
中文翻译:
使用 ELF 测试、FIB-4 和 NAFLD 纤维化评分来筛查人群是否患有肝病
背景与目标
需要准确的纤维化生物标志物来筛查酒精相关和非酒精性脂肪肝病(ALD、NAFLD)。我们使用瞬时弹性成像作为参考标准,将增强肝纤维化 (ELF) 测试的性能与纤维化 4 指数 (FIB-4) 和 NAFLD 纤维化评分 (NFS) 进行比较。
方法
我们前瞻性地纳入了来自普通人群以及有 ALD 或 NAFLD 风险的人群。筛选阳性参与者(TE ≥8 kPa)接受肝活检。我们使用经过验证的临界值测量了伴随的 ELF、FIB-4 和 NFS:分别≥9.8、≥1.3、≥-1.45。
结果
我们纳入了 3,378 名参与者(1,973 名普通人群,953 名有 ALD 风险,452 名有 NAFLD 风险),中位年龄为 57 岁(IQR:51-63)。242 例筛查呈阳性(普通人群中 3.4%,有 ALD/NAFLD 风险的人群分别为 12%/14%)。尽管 ELF 和 TE 之间的总体相关性较差(Spearman´s rho = 0.207),但大多数 TE <8 kPa 的参与者的 ELF <9.8 (88%)。ELF 的假阳性率 (11%) 显着低于 FIB-4 和 NFS(35% 和 45%),同时假阴性率较低(<8%)。在不确定病例中采用 FIB-4 和 ELF 筛查策略导致 8% 的假阳性、4% 的假阴性以及 88% 的病例正确分类。我们对 155/242 (64%) 筛查呈阳性的患者进行了肝活检,其中 54 名 (35%) 患有晚期纤维化 (≥F3)。ELF 诊断晚期纤维化的诊断准确性明显高于 FIB-4 和 NFS:AUROC 分别为 0.85 (95% CI 0.79-0.92) vs. 0.73 (0.64-0.81) 和 0.66 (0.57-0.76)。
结论
与 FIB-4 和 NFS 相比,单独使用 ELF 测试或与 FIB-4 结合进行普通人群和高危人群的肝纤维化筛查可减少无效转诊的数量,同时不会忽视真实病例。
影响和影响
我们需要有效检测人群中酒精相关性和非酒精性脂肪肝病引起的晚期纤维化的转诊途径,但不会导致无效的转诊或过度使用资源。这项研究表明,在不确定的病例中,先进行 FIB-4 顺序检测,然后进行 ELF 检测,导致很少有患者转诊进行确认性肝硬度测量,同时保留了较高的检测病例率,且直接成本较低。这种两步转诊途径可用于初级保健对人群中肝纤维化的大规模、有针对性或机会性筛查。
临床试验编号
ClinicalTrials.gov 编号 NCT03308916。










































 京公网安备 11010802027423号
京公网安备 11010802027423号