Annals of Intensive Care ( IF 5.7 ) Pub Date : 2022-09-30 , DOI: 10.1186/s13613-022-01059-9 Paul Chabert 1, 2 , Judith Provoost 1 , Sabine Cohen 3 , Céline Dupieux-Chabert 4 , Laurent Bitker 1, 5, 6, 7 , Tristan Ferry 2, 5, 6 , Sylvain Goutelle 5, 6, 8, 9 , Jean-Christophe Richard 1, 5, 6, 7
|
Background
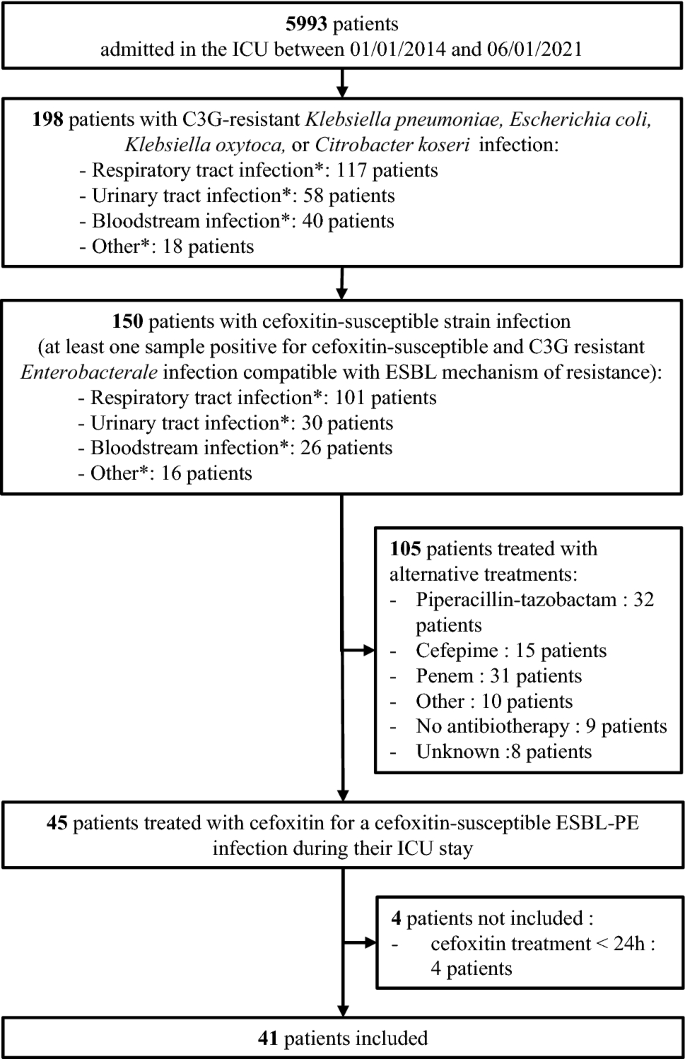
Cefoxitin is active against some extended-spectrum beta-lactamase-producing Enterobacterales (ESBL-PE), but has not been evaluated so far in the intensive care unit (ICU) settings. Data upon its pharmacokinetics (PK), tolerance and efficacy in critical conditions are scanty. We performed a retrospective single-center study in a university hospital medical ICU, in subjects presenting with cefoxitin-susceptible ESBL-PE infection and treated with cefoxitin. The primary aim was to determine cefoxitin PK. Secondary endpoints were efficacy, tolerance, and emergence of cephamycin-resistance.
Results
Forty-one patients were included in this study, mainly with ESBL-PE pneumonia (35 patients, 85%). Cefoxitin was administered during a median [interquartile range (IQR)] duration of 5 [4–7] days. Cefoxitin serum concentrations strongly depended on renal function. Target serum concentration (> 5 × minimum inhibitory concentration (MIC) 24 h after cefoxitin onset was obtained in 34 patients (83%), using a median [IQR] daily dose of 6 [6–6] g with continuous administration. The standard dosage of 6 g/24 h was not sufficient to achieve the PK/PD target serum concentration for MIC up to 4–8 mg/L, except in patients with severe renal impairment and those treated with renal replacement therapy. Treatment failure occurred in 26 cases (63%), among whom 12 patients (29%) died, 13 patients (32%) were switched to alternative antibiotic therapy and 11 patients (27%) presented with relapse of infection with the same ESBL-PE. Serious adverse events attributed to cefoxitin occurred in 7 patients (17%). Acquisition of cephamycin-resistance with the same Enterobacterales was identified in 13 patients (32%), and was associated with underdosage.
Conclusion
Continuous administration of large doses of cefoxitin appears necessary to achieve the PK/PD target in patients with normal renal function. Renal status, MIC determination and therapeutic drug monitoring may be useful for treatment individualization in this setting. The treatment failure rate was 63%. The cefoxitin safety profile was favorable, but we observed a high rate of cephamycin-resistance emergence.
中文翻译:
头孢西丁治疗危重患者对头孢西丁敏感的产超广谱β-内酰胺酶肠杆菌感染的药代动力学、疗效和耐受性:一项回顾性单中心研究
背景
头孢西丁对一些产超广谱 β-内酰胺酶的肠杆菌(ESBL-PE) 有活性,但目前尚未在重症监护室 (ICU) 环境中进行评估。关于其在危急条件下的药代动力学(PK)、耐受性和功效的数据很少。我们在一所大学医院内科 ICU 中进行了一项回顾性单中心研究,研究对象为头孢西丁易感 ESBL-PE 感染并接受头孢西丁治疗的受试者。主要目的是确定头孢西丁 PK。次要终点是疗效、耐受性和头霉素耐药性的出现。
结果
本研究共纳入 41 名患者,主要为 ESBL-PE 肺炎(35 名患者,85%)。在 5 [4-7] 天的中位 [四分位距 (IQR)] 持续时间内给予头孢西丁。头孢西丁血清浓度强烈依赖于肾功能。在 34 名患者 (83%) 中获得头孢西丁起效后 24 小时的目标血清浓度(> 5 × 最低抑菌浓度 (MIC),中位 [IQR] 日剂量为 6 [6-6] g,持续给药。标准6 g/24 h 的剂量不足以达到 PK/PD 目标血清浓度,使 MIC 达到 4-8 mg/L,严重肾功能不全患者和接受肾脏替代治疗的患者除外。治疗失败发生在 26例(63%),其中 12 例(29%)死亡,13 名患者 (32%) 改用替代抗生素治疗,11 名患者 (27%) 因相同的 ESBL-PE 感染复发。7 名患者(17%)发生了归因于头孢西丁的严重不良事件。获得相同的头霉素抗性在 13 名患者 (32%) 中发现了肠杆菌,并且与剂量不足有关。
结论
在肾功能正常的患者中,连续给予大剂量头孢西丁似乎是实现 PK/PD 目标所必需的。在这种情况下,肾脏状况、MIC 测定和治疗药物监测可能有助于治疗个体化。治疗失败率为63%。头孢西丁的安全性良好,但我们观察到头霉素耐药率很高。










































 京公网安备 11010802027423号
京公网安备 11010802027423号