Surgical Endoscopy ( IF 2.4 ) Pub Date : 2022-09-28 , DOI: 10.1007/s00464-022-09649-1 Hyun Jin Bae 1 , Hoyeon Ju 2 , Han Hee Lee 3 , Jinsu Kim 4 , Bo-In Lee 2 , Sung Hak Lee 5 , Daeyoun David Won 6 , Yoon Suk Lee 6 , In Kyu Lee 6 , Young-Seok Cho 2
|
Background
The long-term outcomes of patients with T1 colorectal cancer (CRC) who undergo endoscopic and/or surgical treatment are not well understood. Invasive CRC confined to the colonic submucosa (T1 CRC) is challenging in terms of clinical decision-making. We compared the long-term outcomes of T1 CRC by treatment method.
Methods
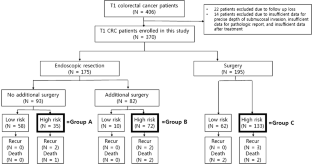
We examined 370 patients with pathological T1 CRC treated between 2000 and 2015 at Seoul St. Mary’s Hospital. In total, 93 patients underwent endoscopic resection (ER) only, 82 underwent additional surgery after ER, and 175 underwent surgical resection only. Patients who did not meet the curative criteria were defined as “high-risk.” High-risk patients were classified into three groups according to the treatment modalities: ER only (Group A: 35 patients), additional surgery after ER (Group B: 72 patients), and surgical resection only (Group C: 133 patients). The recurrence-free and overall survival (OS) rates, and factors associated with recurrence and mortality, were analyzed. Factors associated with lymph node metastasis (LNM) were subjected to multivariate analysis.
Results
Of the 370 patients, 7 experienced recurrence and 7 died. All recurrences occurred in the high-risk group and two deaths were in the low-risk group. In high-risk groups, there was no significant group difference in recurrence-free survival (P = 0.511) or OS (P =0.657). Poor histology (P =0.042) was associated with recurrence, and vascular invasion (P =0.044) with mortality. LNMs were observed in 30 of 277 patients who underwent surgery either initially or secondarily. Lymphatic invasion was significantly associated with the incidence of LNM (P < 0.001).
Conclusions
ER prior to surgery did not affect the prognosis of high-risk T1 CRC patients, and did not worsen the clinical outcomes of patients who required additional surgery. Lymphatic invasion was the most important predictor of LNM.
中文翻译:
内镜与手术切除 T1 期结直肠癌后的长期结果
背景
接受内镜和/或手术治疗的 T1 期结直肠癌 (CRC) 患者的长期结果尚不清楚。局限于结肠粘膜下层的侵袭性 CRC (T1 CRC) 在临床决策方面具有挑战性。我们通过治疗方法比较了 T1 CRC 的长期结果。
方法
我们检查了 2000 年至 2015 年间在首尔圣玛丽医院接受治疗的 370 名病理性 T1 CRC 患者。总共有 93 名患者仅接受了内镜下切除术 (ER),82 名患者在 ER 后接受了额外的手术,175 名患者仅接受了手术切除。不符合治愈标准的患者被定义为“高风险”。根据治疗方式将高危患者分为三组:仅 ER(A 组:35 名患者)、ER 后再次手术(B 组:72 名患者)和仅手术切除(C 组:133 名患者)。分析了无复发和总生存 (OS) 率,以及与复发和死亡率相关的因素。对与淋巴结转移 (LNM) 相关的因素进行多变量分析。
结果
370 例患者中,7 例复发,7 例死亡。所有复发均发生在高风险组,2 例死亡发生在低风险组。在高危组中,无复发生存率 ( P = 0.511) 或 OS ( P =0.657) 无显着组间差异。组织学差 ( P =0.042) 与复发相关,血管侵犯 ( P =0.044) 与死亡率相关。在初次或二次接受手术的 277 名患者中,有 30 名观察到 LNM。淋巴管侵犯与 LNM 的发生显着相关(P < 0.001)。
结论
术前 ER 不影响高危 T1 CRC 患者的预后,也不会恶化需要额外手术的患者的临床结果。淋巴侵犯是 LNM 最重要的预测因子。










































 京公网安备 11010802027423号
京公网安备 11010802027423号