Skeletal Radiology ( IF 1.9 ) Pub Date : 2022-09-26 , DOI: 10.1007/s00256-022-04191-6 Frank W Roemer 1, 2 , Mohamed Jarraya 3 , Jamie E Collins 4 , C Kent Kwoh 5 , Daichi Hayashi 6 , David J Hunter 7 , Ali Guermazi 1, 8
|
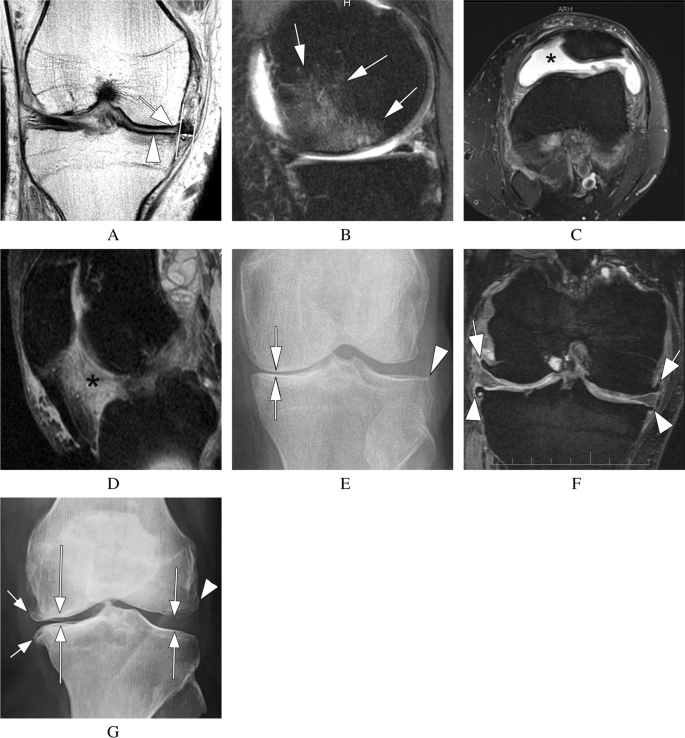
A joint contains many different tissues that can exhibit pathological changes, providing many potential targets for treatment. Researchers are increasingly suggesting that osteoarthritis (OA) comprises several phenotypes or subpopulations. Consequently, a treatment for OA that targets only one pathophysiologic abnormality is unlikely to be similarly efficacious in preventing or delaying the progression of all the different phenotypes of structural OA. Five structural phenotypes have been proposed, namely the inflammatory, meniscus-cartilage, subchondral bone, and atrophic and hypertrophic phenotypes. The inflammatory phenotype is characterized by marked synovitis and/or joint effusion, while the meniscus-cartilage phenotype exhibits severe meniscal and cartilage damage. Large bone marrow lesions characterize the subchondral bone phenotype. The hypertrophic and atrophic OA phenotype are defined based on the presence large osteophytes or absence of any osteophytes, respectively, in the presence of concomitant cartilage damage. Limitations of the concept of structural phenotyping are that they are not mutually exclusive and that more than one phenotype may be present. It must be acknowledged that a wide range of views exist on how best to operationalize the concept of structural OA phenotypes and that the concept of structural phenotypic characterization is still in its infancy. Structural phenotypic stratification, however, may result in more targeted trial populations with successful outcomes and practitioners need to be aware of the heterogeneity of the disease to personalize their treatment recommendations for an individual patient. Radiologists should be able to define a joint at risk for progression based on the predominant phenotype present at different disease stages.
中文翻译:
膝骨关节炎的结构表型:潜在的临床和研究相关性
关节包含许多不同的组织,可以表现出病理变化,为治疗提供许多潜在的靶点。研究人员越来越多地认为骨关节炎 (OA) 包含多种表型或亚群。因此,仅针对一种病理生理异常的 OA 治疗不太可能在预防或延缓结构性 OA 的所有不同表型的进展方面同样有效。已经提出了五种结构表型,即炎症表型、半月板软骨、软骨下骨以及萎缩和肥大表型。炎症表型的特征是明显的滑膜炎和/或关节积液,而半月板-软骨表型则表现出严重的半月板和软骨损伤。大骨髓病变是软骨下骨表型的特征。肥大性和萎缩性 OA 表型分别根据存在大骨赘或不存在任何骨赘,同时伴有软骨损伤来定义。结构表型概念的局限性在于它们不是相互排斥的并且可能存在不止一种表型。必须承认,对于如何最好地运用结构 OA 表型的概念存在着广泛的观点,并且结构表型表征的概念仍处于起步阶段。然而,结构表型分层可能会导致更有针对性的试验人群获得成功的结果,并且从业者需要意识到疾病的异质性,以便为个体患者提供个性化的治疗建议。放射科医生应该能够根据不同疾病阶段存在的主要表型来定义有进展风险的关节。










































 京公网安备 11010802027423号
京公网安备 11010802027423号