Pediatric Nephrology ( IF 2.6 ) Pub Date : 2022-08-22 , DOI: 10.1007/s00467-022-05706-y Ann Christin Gjerstad 1 , Rannveig Skrunes 2, 3 , Camilla Tøndel 4, 5 , Anders Åsberg 6, 7, 8 , Sabine Leh 3, 9 , Claus Klingenberg 10, 11 , Henrik Døllner 12, 13 , Clara Hammarstrøm 14 , Anna Kristina Bjerre 1, 15
|
Background
There is scarce information on biopsy-verified kidney disease in childhood and its progression to chronic kidney disease stage 5 (CKD 5). This study aims to review biopsy findings in children, and to investigate risk of kidney replacement therapy (KRT).
Methods
We conducted a retrospective long-term follow-up study of children included in the Norwegian Kidney Biopsy Registry (NKBR) and in the Norwegian Renal Registry (NRR) from 1988 to 2021.
Results
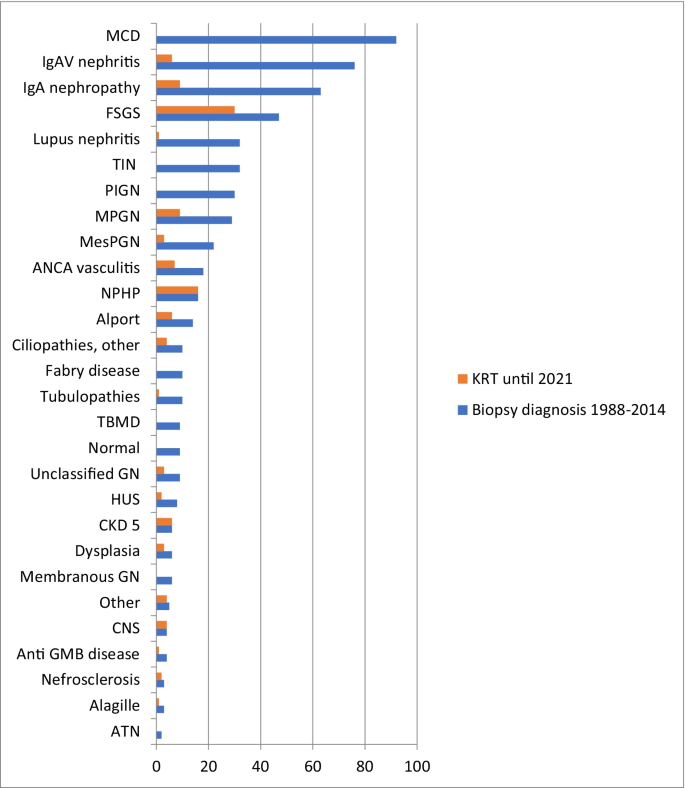
In total, 575 children with a median (interquartile range, IQR) age of 10.7 (6.1 to 14.1) years were included, and median follow-up time (IQR) after kidney biopsy was 14.3 (range 8.9 to 21.6) years. The most common biopsy diagnoses were minimal change disease (MCD; n = 92), IgA vasculitis nephritis (IgAVN; n = 76), IgA nephropathy (n = 63), and focal and segmental glomerulosclerosis (FSGS; n = 47). In total, 118 (20.5%) of the biopsied children reached CKD 5, median (IQR) time to KRT 2.3 years (7 months to 8.4 years). Most frequently, nephronophthisis (NPHP; n = 16), FSGS (n = 30), IgA nephropathy (n = 9), and membranoproliferative glomerulonephritis (MPGN; n = 9) led to KRT.
Conclusions
The risk of KRT after a kidney biopsy diagnosis is highly dependent on the diagnosis. None of the children with MCD commenced KRT, while 63.8% with FSGS and 100% with NPHP reached KRT. Combining data from kidney biopsy registries with registries on KRT allows for detailed information concerning the risk for later CKD 5 after biopsy-verified kidney disease in childhood.
Graphical abstract
A higher resolution version of the Graphical abstract is available as Supplementary information
中文翻译:
挪威肾脏活检登记处儿童期肾脏活检诊断和肾脏替代治疗的长期风险:25 年随访
背景
关于经活检证实的儿童肾病及其进展为慢性肾病 5 期 (CKD 5) 的信息很少。本研究旨在回顾儿童的活检结果,并调查肾脏替代疗法 (KRT) 的风险。
方法
我们对 1988 年至 2021 年挪威肾脏活检登记处 (NKBR) 和挪威肾脏登记处 (NRR) 中的儿童进行了一项回顾性长期随访研究。
结果
总共纳入了 575 名中位(四分位数间距,IQR)年龄为 10.7(6.1 至 14.1)岁的儿童,肾活检后的中位随访时间 (IQR) 为 14.3(范围 8.9 至 21.6)年。最常见的活检诊断是微小病变(MCD;n = 92)、IgA 血管炎性肾炎(IgAVN;n = 76)、IgA 肾病(n = 63)和局灶节段性肾小球硬化症(FSGS;n = 47)。总共有 118 名 (20.5%) 的活检儿童达到 CKD 5,中位 (IQR) 时间至 KRT 为 2.3 年(7 个月至 8.4 年)。最常见的是肾病(NPHP;n = 16)、FSGS(n = 30)、IgA 肾病(n = 9), 和膜增生性肾小球肾炎 (MPGN; n = 9) 导致 KRT。
结论
肾活检诊断后 KRT 的风险在很大程度上取决于诊断。没有 MCD 儿童开始 KRT,而 63.8% 的 FSGS 和 100% 的 NPHP 儿童达到了 KRT。将肾活检登记处的数据与 KRT 登记处的数据相结合,可以提供有关儿童活检证实的肾脏疾病后发生 CKD 5 的风险的详细信息。
图形概要
图形摘要的更高分辨率版本可作为补充信息使用









































 京公网安备 11010802027423号
京公网安备 11010802027423号