Clinical Pharmacokinetics ( IF 4.5 ) Pub Date : 2022-07-25 , DOI: 10.1007/s40262-022-01147-w James D Chalmers 1 , Helen Usansky 2 , Christopher M Rubino 3 , Ariel Teper 2 , Carlos Fernandez 2 , Jun Zou 2 , Kevin C Mange 2
|
Background and Objective
Brensocatib is an investigational, first-in-class, selective, and reversible dipeptidyl peptidase 1 inhibitor that blocks activation of neutrophil serine proteases (NSPs). The NSPs neutrophil elastase, cathepsin G, and proteinase 3 are believed to be central to the pathogenesis of several chronic inflammatory diseases, including bronchiectasis. In a phase II study, oral brensocatib 10 mg and 25 mg reduced sputum neutrophil elastase activity and prolonged the time to pulmonary exacerbation in patients with non-cystic fibrosis bronchiectasis (NCFBE). A population pharmacokinetic (PPK) model was developed to characterize brensocatib exposure, determine potential relationships between brensocatib exposure and efficacy and safety measures, and inform dose selection in clinical studies.
Methods
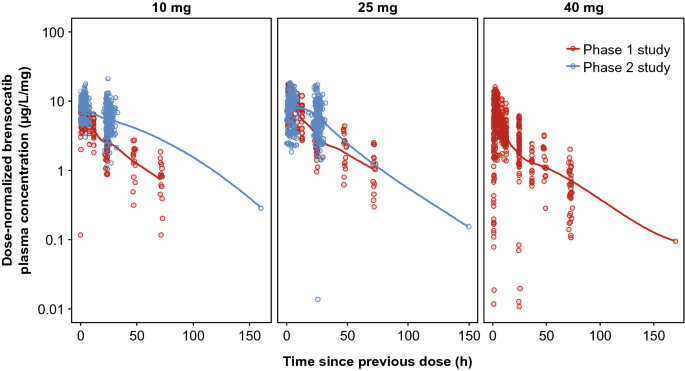
Pharmacokinetic (PK) data pooled from a phase I study of once-daily brensocatib (10, 25, and 40 mg) in healthy adults and a phase II study of once-daily brensocatib (10 mg and 25 mg) in adults with NCFBE were used to develop a PPK model and to evaluate potential covariate effects on brensocatib pharmacokinetics. PK–efficacy relationships for sputum neutrophil elastase below the level of quantification (BLQ) and reduction in pulmonary exacerbation and PK–safety relationships for adverse events of special interest (AESIs; periodontal disease, hyperkeratosis, and infections other than pulmonary infections) were evaluated based on model-predicted brensocatib exposure. A total of 1284 steady-state brensocatib concentrations from 225 individuals were included in the PPK data set; 241 patients with NCFBE from the phase II study were included in the pharmacodynamic (PD) population for the PK/PD analyses.
Results
The PPK model that best described the observed data consisted of two distributional compartments and linear clearance. Two significant covariates were found: age on volume of distribution and renal function on apparent oral clearance. PK–efficacy analysis revealed a threshold brensocatib exposure (area under the concentration–time curve) effect for attaining sputum neutrophil elastase BLQ and a strong relationship between sputum neutrophil elastase BLQ and reduction in pulmonary exacerbations. A PK–safety evaluation showed no noticeable trends between brensocatib exposure and the incidence of AESIs. Based on the predicted likelihood of clinical outcomes for sputum neutrophil elastase BLQ and pulmonary exacerbations, brensocatib doses of 10 mg and 25 mg once daily were selected for a phase III clinical trial in patients with NCFBE (ClinicalTrials.gov identifier: NCT04594369).
Conclusions
PPK results revealed that age and renal function have a moderate effect on brensocatib exposure. However, this finding does not warrant dose adjustments based on age or in those with mild or moderate renal impairment. The PK/PD evaluation demonstrated the clinically meaningful relationship between suppression of neutrophil elastase activity and reduction in exacerbations in brensocatib-treated patients with NCFBE, supporting further development of brensocatib for bronchiectasis.
中文翻译:
二肽基肽酶 1 抑制剂 Brensocatib 治疗非囊性纤维化支气管扩张的药代动力学/药效学评价
背景和目标
Brensocatib 是一种研究性、一流的、选择性的、可逆的二肽基肽酶 1 抑制剂,可阻断中性粒细胞丝氨酸蛋白酶 (NSP) 的激活。NSPs 中性粒细胞弹性蛋白酶、组织蛋白酶 G 和蛋白酶 3 被认为是包括支气管扩张症在内的多种慢性炎症性疾病发病机制的核心。在一项 II 期研究中,口服 brensocatib 10 mg 和 25 mg 可降低非囊性纤维化支气管扩张症 (NCFBE) 患者的痰液中性粒细胞弹性蛋白酶活性并延长至肺部恶化的时间。开发了一种群体药代动力学 (PPK) 模型来表征 brensocatib 暴露,确定 brensocatib 暴露与疗效和安全措施之间的潜在关系,并为临床研究中的剂量选择提供信息。
方法
药代动力学 (PK) 数据汇集自健康成人每天一次 brensocatib(10、25 和 40 mg)的 I 期研究和 NCFBE 成人每天一次 brensocatib(10 mg 和 25 mg)的 II 期研究用于开发 PPK 模型并评估对 brensocatib 药代动力学的潜在协变量影响。低于定量水平 (BLQ) 的痰中性粒细胞弹性蛋白酶的 PK-功效关系和肺部恶化的减少以及特别关注的不良事件(AESI;牙周病、角化过度和肺部感染以外的感染)的 PK-安全关系是基于关于模型预测的 brensocatib 暴露。PPK 数据集中包含来自 225 个个体的总共 1284 个稳态 brensocatib 浓度;
结果
最能描述观察到的数据的 PPK 模型由两个分布区室和线性间隙组成。发现了两个显着的协变量:分布容积的年龄和表观口服清除率的肾功能。PK 疗效分析揭示了达到痰中性粒细胞弹性蛋白酶 BLQ 的阈值 brensocatib 暴露(浓度-时间曲线下面积)效应,以及痰中性粒细胞弹性蛋白酶 BLQ 与肺部恶化减少之间的密切关系。PK-安全性评估显示 brensocatib 暴露与 AESI 发生率之间没有明显趋势。根据痰液中性粒细胞弹性蛋白酶 BLQ 和肺部恶化的临床结果的预测可能性,选择每天一次 10 mg 和 25 mg 剂量的 brensocatib 用于 NCFBE 患者的 III 期临床试验(ClinicalTrials.
结论
PPK 结果显示年龄和肾功能对 brensocatib 暴露有中度影响。然而,这一发现并不能保证根据年龄或轻度或中度肾功能不全患者进行剂量调整。PK/PD 评估表明,在接受 brensocatib 治疗的 NCFBE 患者中,抑制中性粒细胞弹性蛋白酶活性与减少急性加重之间存在具有临床意义的关系,支持进一步开发 brensocatib 治疗支气管扩张症。


























 京公网安备 11010802027423号
京公网安备 11010802027423号