Clinical Pharmacokinetics ( IF 4.6 ) Pub Date : 2022-08-16 , DOI: 10.1007/s40262-022-01168-5 Romain Garreau 1, 2 , Damien Montange 3, 4 , Antoine Grillon 5 , François Jehl 5 , Tristan Ferry 6, 7, 8 , Laurent Bourguignon 1, 2, 7 , Sylvain Goutelle 1, 2, 7
|
Background and Objective
Daptomycin has been recommended in the treatment of bone and joint infection. Previous work showed that the approved dosage of daptomycin may be insufficient to achieve optimal exposure in patients with bone and joint infection. However, those studies assumed that bone exposure was similar to steady-state daptomycin-free plasma concentrations. We sought to establish a physiologically based pharmacokinetic (PBPK) model of daptomycin to describe the dynamics of daptomycin disposition in bone and skin tissue.
Methods
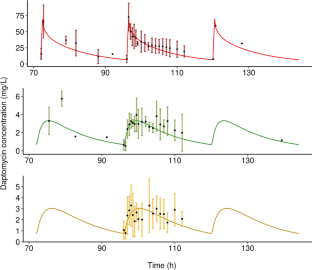
A PBPK model of daptomycin was built using PK-Sim®. Daptomycin concentrations in plasma and bone were obtained from three previously published studies. Physicochemical drug characteristics, mass balance, anthropometrics, and experimental data were used to build and refine the PBPK model. Internal validation of the PBPK model was performed using the usual diagnostic plots. The final PBPK model was then used to run simulations with doses of 6, 8, 10, and 12 mg/kg/24 h. Pharmacokinetic profiles were simulated in 1000 subjects and the probabilities of target attainment for the area under the concentration–time curve over the bacterial minimum inhibitory concentration were computed in blood, skin, and bone compartments.
Results
The final model showed a good fit of all datasets with an absolute average fold error between 0.5 and 2 for all pharmacokinetic quantities in blood, skin and bone tissues. Results of dosing simulations showed that doses ≥10 mg/kg should be used in the case of bacteremia caused by Staphylococcus aureus with a minimum inhibitory concentration >0.5 mg/L or Enterococcus faecalis with a minimum inhibitory concentration >1 mg/L, while doses ≥12 mg/kg should be used in the case of bone and joint infection or complicated skin infection. When considering a lower minimum inhibitory concentration, doses of 6–8 mg/kg would likely achieve a sufficient success rate. However, in the case of infections caused by E. faecalis with a minimum inhibitory concentration >2 mg/L, a higher dosage and combination therapy would be necessary to maximize efficacy.
Conclusions
We developed the first daptomycin PBPK/pharmacodynamic model for bone and joint infection, which confirmed that a higher daptomycin dosage is needed to optimize exposure in bone tissue. However, such higher dosages raise safety concerns. In this setting, therapeutic drug monitoring and model-informed precision dosing appear necessary to ensure the right exposure on an individual basis.
中文翻译:
基于达托霉素生理学的药代动力学模型预测皮肤和骨骼组织中的药物暴露和药效学
背景和目标
达托霉素已被推荐用于治疗骨和关节感染。以前的工作表明,批准的达托霉素剂量可能不足以在骨和关节感染患者中达到最佳暴露。然而,这些研究假设骨暴露与稳态无达托霉素血浆浓度相似。我们试图建立达托霉素的生理学药代动力学 (PBPK) 模型来描述达托霉素在骨骼和皮肤组织中的分布动力学。
方法
使用 PK-Sim ®建立了达托霉素的 PBPK 模型。达托霉素在血浆和骨骼中的浓度是从之前发表的三项研究中获得的。使用理化药物特性、质量平衡、人体测量学和实验数据来建立和改进 PBPK 模型。使用通常的诊断图对 PBPK 模型进行内部验证。然后使用最终的 PBPK 模型以 6、8、10 和 12 mg/kg/24 h 的剂量运行模拟。在 1000 名受试者中模拟了药代动力学曲线,并计算了血液、皮肤和骨骼隔室中浓度-时间曲线下面积相对于细菌最小抑菌浓度的目标实现概率。
结果
最终模型显示了所有数据集的良好拟合,对于血液、皮肤和骨组织中的所有药代动力学量,绝对平均倍数误差在 0.5 到 2 之间。给药模拟结果表明,对于最低抑菌浓度>0.5 mg/L的金黄色葡萄球菌或最低抑菌浓度>1 mg/L的粪肠球菌引起的菌血症,应使用≥10 mg/kg的剂量,而剂量骨关节感染或并发皮肤感染者应使用≥12mg/kg。当考虑较低的最低抑制浓度时,6–8 mg/kg 的剂量可能会达到足够的成功率。然而,在由粪肠球菌引起的感染的情况下如果最低抑菌浓度 >2 mg/L,则需要更高的剂量和联合治疗才能最大限度地提高疗效。
结论
我们开发了第一个用于骨和关节感染的达托霉素 PBPK/药效学模型,证实需要更高的达托霉素剂量来优化骨组织中的暴露。然而,如此高的剂量会引起安全问题。在这种情况下,治疗药物监测和基于模型的精确剂量似乎是确保个体正确暴露的必要条件。










































 京公网安备 11010802027423号
京公网安备 11010802027423号