The Journal of Heart and Lung Transplantation ( IF 6.4 ) Pub Date : 2022-08-15 , DOI: 10.1016/j.healun.2022.08.006 Raymond L Benza 1 , Mardi Gomberg-Maitland 2 , Harrison W Farber 3 , Carmine Dario Vizza 4 , Meredith Broderick 5 , Louis Holdstock 5 , Andrew C Nelsen 5 , Chunqin Deng 5 , Youlan Rao 5 , R James White 6
|
Background
Risk scores integrate clinical variables emphasizing symptoms, exercise capacity, and measures of cardiac strain to predict clinical outcome better than any single value in pulmonary arterial hypertension (PAH). Risk scores have demonstrated prognostic utility for outcomes in registries, and recent studies have suggested that they are also therapy-responsive in controlled trials.
Methods
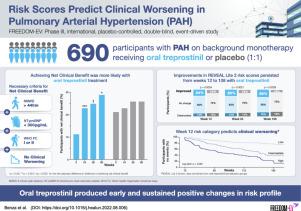
FREEDOM-EV, a global, placebo-controlled, event-driven study, randomized 690 PAH participants 1:1 to oral treprostinil (TRE) or placebo. Clinical assessments were performed every 12 weeks to calculate the non-invasive French risk assessment (FRA), 4-strata COMPERA, REVEAL 2.0, and REVEAL Lite 2; median follow-up was 58 weeks. The Week 12 risk scores were used to predict time to clinical worsening (from Week 12) with Kaplan-Meier product-limit estimates. Log-rank test was used to calculate the statistical difference among risk categories, and mediation analysis tested the hypothesis that improvements in risk score contributed to reduced likelihood for clinical worsening. We assessed the previously proposed “net clinical benefit” (achievement of FRA low-risk status and absence of clinical worsening).
Results
Both REVEAL scores, COMPERA, and FRA at Week 12 predicted subsequent clinical worsening better than baseline risk. Mediation analysis demonstrated that Week 12 risk score reduction explained part of TRE's effect on clinical worsening, especially for those with higher baseline risk. TRE assigned participants were more likely to achieve the previously proposed “net clinical benefit” at Weeks 24 and beyond. Few participants who achieved ‘net clinical benefit’ had subsequent clinical worsening.
Conclusions
Contemporary risk scores were therapy responsive in FREEDOM-EV and early improvements predicted subsequent outcomes. This post hoc analysis suggests that risk scores may be a surrogate for clinical worsening.
中文翻译:
当代风险评分预测肺动脉高压的临床恶化 - FREEDOM-EV 的分析
背景
风险评分整合临床变量,强调症状、运动能力和心脏应变的测量,以比肺动脉高压 (PAH) 的任何单一值更好地预测临床结果。风险评分已证明对登记结果的预后效用,最近的研究表明它们在对照试验中也具有治疗反应性。
方法
FREEDOM-EV 是一项全球性、安慰剂对照、事件驱动的研究,将 690 名 PAH 参与者以 1:1 的比例随机分配到口服曲前列环素 (TRE) 或安慰剂组。每 12 周进行一次临床评估,以计算无创法国风险评估 (FRA)、4 层 COMPERA、REVEAL 2.0 和 REVEAL Lite 2;中位随访时间为 58 周。第 12 周的风险评分用于预测临床恶化的时间(从第 12 周开始),采用 Kaplan-Meier 乘积限制估计。对数秩检验用于计算风险类别之间的统计差异,中介分析检验了风险评分的提高有助于降低临床恶化可能性的假设。我们评估了之前提出的“净临床获益”(达到 FRA 低风险状态且没有临床恶化)。
结果
第 12 周的 REVEAL 评分、COMPERA 和 FRA 都比基线风险更能预测随后的临床恶化。中介分析表明,第 12 周的风险评分降低解释了 TRE 对临床恶化的部分影响,特别是对于基线风险较高的患者。TRE 分配的参与者更有可能在第 24 周及以后实现先前提出的“净临床益处”。很少有获得“净临床获益”的参与者随后出现临床恶化。
结论
当代风险评分在 FREEDOM-EV 中对治疗有反应,早期改善预测随后的结果。这项事后分析表明,风险评分可能是临床恶化的替代指标。








































 京公网安备 11010802027423号
京公网安备 11010802027423号