Chest ( IF 9.6 ) Pub Date : 2022-08-08 , DOI: 10.1016/j.chest.2022.08.001 Nicholas A Bosch 1 , Anica C Law 1 , Emily A Vail 2 , Kari R Gillmeyer 1 , Hayley B Gershengorn 3 , Hannah Wunsch 4 , Allan J Walkey 5
|
Background
The inhaled vasodilators nitric oxide and epoprostenol may be initiated to improve oxygenation in mechanically ventilated patients with severe acute respiratory failure (ARF); however, practice patterns and head-to-head comparisons of effectiveness are unclear.
Research Question
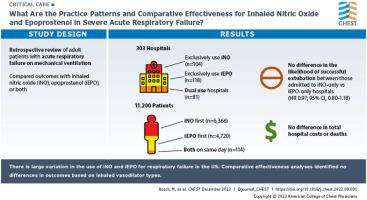
What are the practice patterns and comparative effectiveness for inhaled nitric oxide and epoprostenol in severe ARF?
Study Design and Methods
Using a large US database (Premier Healthcare Database), we identified adult patients with ARF or ARDS who were mechanically ventilated and started on inhaled nitric oxide, epoprostenol, or both. Leveraging large hospital variation in the choice of initial inhaled vasodilator, we compared the effectiveness of inhaled nitric oxide with that of epoprostenol by limiting analysis to patients admitted to hospitals that exclusively used either inhaled nitric oxide or epoprostenol. The primary outcome of successful extubation was modeled using multivariate Fine-Grey competing risk (death or hospice discharge) time-to-event models.
Results
Among 11,200 patients (303 hospitals), 6,366 patients (56.8%) received inhaled nitric oxide first, 4,720 patients (42.1%) received inhaled epoprostenol first, and 114 patients (1.0%) received both therapies on the same day. One hundred four hospitals (34.3%; 1,666 patients) exclusively used nitric oxide and 118 hospitals (38.9%; 1,812 patients) exclusively used epoprostenol. No differences were found in the likelihood of successful extubation between patients admitted to nitric oxide-only hospitals vs those admitted to epoprostenol-only hospitals (subdistribution hazard ratio, 0.97; 95% CI, 0.80-1.18). Also no differences were found in total hospital costs or death. Results were robust to multiple sensitivity analyses.
Interpretation
Large variation exists in the use of initial inhaled vasodilator for respiratory failure across US hospitals. Comparative effectiveness analyses identified no differences in outcomes based on inhaled vasodilator type.
中文翻译:
急性呼吸衰竭期间吸入一氧化氮与依前列醇
背景
吸入性血管扩张剂一氧化氮和依前列醇可用于改善严重急性呼吸衰竭 (ARF) 机械通气患者的氧合;然而,实践模式和有效性的直接比较尚不清楚。
研究问题
严重 ARF 中吸入一氧化氮和依前列醇的实践模式和比较有效性是什么?
研究设计和方法
使用大型美国数据库(Premier Healthcare Database),我们确定了接受机械通气并开始吸入一氧化氮、依前列醇或两者的成年 ARF 或 ARDS 患者。利用医院在选择初始吸入性血管扩张剂方面的巨大差异,我们通过将分析限制在仅使用吸入性一氧化氮或依前列醇的医院收治的患者,比较了吸入性一氧化氮与依前列醇的有效性。使用多变量 Fine-Grey 竞争风险(死亡或临终关怀出院)事件发生时间模型对成功拔管的主要结果进行建模。
结果
在 11,200 名患者(303 家医院)中,6,366 名患者 (56.8%) 首先接受吸入一氧化氮,4,720 名患者 (42.1%) 首先接受吸入依前列醇,114 名患者 (1.0%) 在同一天接受两种治疗。104 家医院(34.3%;1,666 名患者)专门使用一氧化氮,118 家医院(38.9%;1,812 名患者)专门使用依前列醇。入住仅一氧化氮医院的患者与入住仅依前列醇医院的患者之间成功拔管的可能性没有差异(次分布风险比,0.97;95% CI,0.80-1.18)。在总住院费用或死亡方面也没有发现差异。结果对多重敏感性分析是稳健的。
解释
美国各家医院对呼吸衰竭初始吸入性血管扩张剂的使用存在很大差异。比较有效性分析未发现基于吸入血管扩张剂类型的结果存在差异。


























 京公网安备 11010802027423号
京公网安备 11010802027423号