Pediatric Nephrology ( IF 2.6 ) Pub Date : 2022-08-09 , DOI: 10.1007/s00467-022-05708-w Kevin A Pettit 1 , David T Selewski 2 , David J Askenazi 3 , Rajit K Basu 4 , Brian C Bridges 5 , David S Cooper 6 , Geoffrey M Fleming 5 , Jason Gien 1 , Stephen M Gorga 7 , Jennifer G Jetton 8 , Eileen C King 9 , Heidi J Steflik 2 , Matthew L Paden 10 , Rashmi D Sahay 9 , Michael Zappitelli 11 , Katja M Gist 6
|
Background
Acute kidney injury (AKI) and fluid overload (FO) are associated with poor outcomes in children receiving extracorporeal membrane oxygenation (ECMO). Our objective is to evaluate the impact of AKI and FO on pediatric patients receiving ECMO for cardiac pathology.
Methods
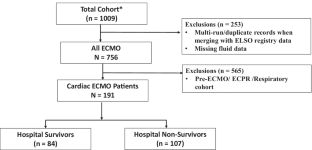
We performed a secondary analysis of the six-center Kidney Interventions During Extracorporeal Membrane Oxygenation (KIDMO) database, including only children who underwent ECMO for cardiac pathology. AKI was defined using Kidney Disease: Improving Global Outcomes (KDIGO) creatinine criteria. FO was defined as < 10% (FO–) vs. ≥ 10% (FO +) and was evaluated at ECMO initiation, peak during ECMO, and ECMO discontinuation. Primary outcomes were mortality and length of stay (LOS).
Results
Data from 191 patients were included. Non-survivors (56%) were more likely to be FO + than survivors at peak ECMO fluid status and ECMO discontinuation. There was a significant interaction between AKI and FO. In the presence of AKI, the adjusted odds of mortality for FO + was 4.79 times greater than FO– (95% CI: 1.52–15.12, p = 0.01). In the presence of FO + , the adjusted odds of mortality for AKI + was 2.7 times higher than AKI– [95%CI: 1.10–6.60; p = 0.03]. Peak FO + was associated with a 55% adjusted relative increase in LOS [95%CI: 1.07–2.26, p = 0.02].
Conclusions
The association of peak FO + with mortality is present only in the presence of AKI + . Similarly, AKI + is associated with mortality only in the presence of peak FO + . FO + was associated with LOS. Studies targeting fluid management have the potential to improve LOS and mortality outcomes.
Graphical abstract
A higher resolution version of the Graphical abstract is available as Supplementary information.
中文翻译:
液体超负荷和急性肾损伤对儿科心脏 ECMO 结果的协同关联:KIDMO 数据库的回顾性分析
背景
急性肾损伤 (AKI) 和体液超负荷 (FO) 与接受体外膜肺氧合 (ECMO) 的儿童预后不良有关。我们的目标是评估 AKI 和 FO 对接受 ECMO 治疗心脏病的儿科患者的影响。
方法
我们对体外膜肺氧合 (KIDMO) 数据库中的六中心肾脏干预进行了二次分析,其中仅包括接受 ECMO 治疗心脏病的儿童。AKI 是使用肾脏疾病:改善全球预后 (KDIGO) 肌酐标准定义的。FO 定义为 < 10% (FO–) 与 ≥ 10% (FO +),并在 ECMO 启动、ECMO 期间达到峰值和 ECMO 停止时进行评估。主要结果是死亡率和住院时间 (LOS)。
结果
包括 191 名患者的数据。在 ECMO 液体状态峰值和 ECMO 停止时,非幸存者 (56%) 比幸存者更有可能出现 FO +。AKI 和 FO 之间存在显着的相互作用。在存在 AKI 的情况下,FO + 的调整死亡率比 FO- 高 4.79 倍(95% CI:1.52–15.12,p = 0.01)。在存在 FO + 的情况下,AKI + 的调整死亡率比 AKI- 高 2.7 倍 [95%CI:1.10–6.60;p = 0.03]。峰值 FO + 与 LOS 调整后 55% 的相对增加相关 [95%CI:1.07–2.26,p = 0.02]。
结论
峰值 FO + 与死亡率的关联仅存在于 AKI + 的情况下。同样,AKI + 仅在存在峰值 FO + 时才与死亡率相关。FO + 与 LOS 相关。针对液体管理的研究有可能改善 LOS 和死亡率结果。
图形概要
图形摘要的更高分辨率版本可作为补充信息使用。










































 京公网安备 11010802027423号
京公网安备 11010802027423号