Pediatric Drugs ( IF 3.4 ) Pub Date : 2022-08-06 , DOI: 10.1007/s40272-022-00524-z Dietmar Schranz 1
|
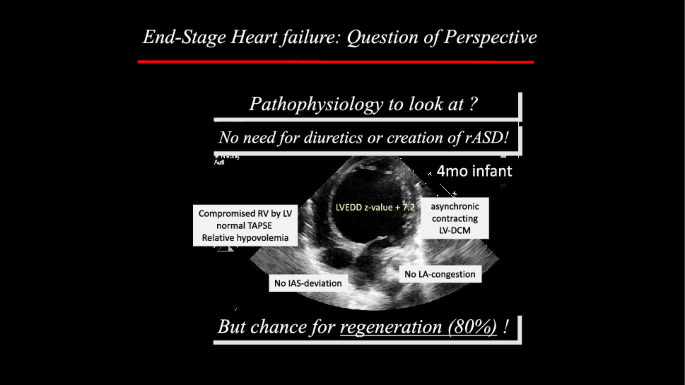
Given the heterogenous etiology of pediatric heart failure (pHF), evidence-based studies improving pHF are unlikely. A paradigm shift towards updated medicine-based evidence is therefore necessary. In view of the life expectancy of children, cardiac regeneration strategies are required. Therefore, age- and disease-related differences in myocardial (receptor) physiology require individualized precision medicine. First-line diuretic therapy, adopted from the treatment of adults with HF with no chance for recovery, should be questioned in the treatment of pHF with potential for recovery. Inadequate use of diuretics is a common reason for additional stimulation of the neurohumoral axis. Consecutive intravascular volume depletion led to an inadequate treatment with β-blocker and renin–angiotensin–aldosterone antagonists. Given the age-related catecholamine-driven cardiovascular (patho-) physiology, highly selective β1-blockers (bisoprolol) protect against β1-(noradrenaline)-related myocytic apoptosis and necrosis, but allow β2-receptor-mediated myocardial regeneration. Based on its high safety–efficacy profile with rarely seen adverse effects but easily monitorable efficacy by the surrogate of heart rate (reduction), bisoprolol is our first-line drug in infancy. Reduced heart rate economizes the heart and full body oxygen consumption and extends the diastolic filling and coronary perfusion time. Based on our many years of institutional experience, physicians should be encouraged to use β1-selected blockers in infants with dilated cardiomyopathy and hypoplastic left heart syndrome after stage-1 procedure, but also to treat ventricular septal defects with a significant left-to-right shunt. In summary, individualized pHF therapy is the prerequisite for a causal treatment to improve HF symptoms, but above all for the most functional regeneration possible.
中文翻译:
可以改进小儿心力衰竭治疗吗?是的,它可以,但是……
鉴于小儿心力衰竭 (pHF) 的异质性病因,改善 pHF 的循证研究不太可能。因此,有必要向更新的基于医学的证据转变范式。鉴于儿童的预期寿命,需要心脏再生策略。因此,心肌(受体)生理学与年龄和疾病相关的差异需要个体化的精准医学。一线利尿剂疗法是从治疗没有机会康复的成人心力衰竭中采用的,在治疗有康复潜力的 pHF 时应该受到质疑。利尿剂使用不当是额外刺激神经体液轴的常见原因。连续的血管内容量减少导致 β 受体阻滞剂和肾素-血管紧张素-醛固酮拮抗剂治疗不充分。鉴于年龄相关的儿茶酚胺驱动的心血管(病理)生理学,高选择性 β1 受体阻滞剂(比索洛尔)可防止 β1-(去甲肾上腺素)相关的肌细胞凋亡和坏死,但允许 β2 受体介导的心肌再生。基于其高安全性和有效性特征,很少见的不良反应,但通过心率(降低)的替代指标很容易监测疗效,比索洛尔是我们在婴儿期的一线药物。降低心率可节省心脏和全身耗氧量并延长舒张期充盈和冠状动脉灌注时间。根据我们多年的机构经验,应鼓励医生在患有扩张型心肌病和左心发育不全综合征的 1 期手术后的婴儿中使用 β1 选择性阻滞剂,还可以治疗具有显着左向右分流的室间隔缺损。总之,个体化 pHF 治疗是改善 HF 症状的因果治疗的先决条件,但最重要的是尽可能实现功能性再生。










































 京公网安备 11010802027423号
京公网安备 11010802027423号