Journal of Clinical Monitoring and Computing ( IF 2.0 ) Pub Date : 2022-08-04 , DOI: 10.1007/s10877-022-00897-z Louis Morisson 1, 2 , Mathieu Nadeau-Vallée 1, 2 , Fabien Espitalier 3 , Pascal Laferrière-Langlois 1, 2 , Moulay Idrissi 1 , Nadia Lahrichi 4 , Céline Gélinas 5 , Olivier Verdonck 1, 2 , Philippe Richebé 1, 2
|
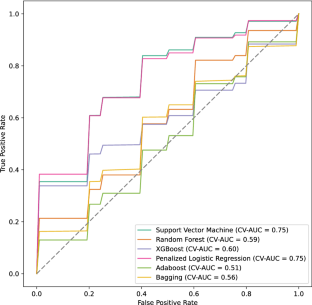
The relationship between intraoperative nociception and acute postoperative pain is still not well established. The nociception level (NOL) Index (Medasense, Ramat Gan, Israel) uses a multiparametric approach to provide a 0–100 nociception score. The objective of the ancillary analysis of the NOLGYN study was to evaluate the ability of a machine-learning aglorithm to predict moderate to severe acute postoperative pain based on intraoperative NOL values. Our study uses the data from the NOLGYN study, a randomized controlled trial that evaluated the impact of NOL-guided intraoperative administration of fentanyl on overall fentanyl consumption compared to standard of care. Seventy patients (ASA class I–III, aged 18–75 years) scheduled for gynecological laparoscopic surgery were enrolled. Variables included baseline demographics, NOL reaction to incision or intubation, median NOL during surgery, NOL time-weighted average (TWA) above or under manufacturers’ recommended thresholds (10–25), and percentage of surgical time spent with NOL > 25 or < 10. We evaluated different machine learning algorithms to predict postoperative pain. Performance was assessed using cross-validated area under the ROC curve (CV-AUC). Of the 66 patients analyzed, 42 (63.6%) experienced moderate to severe pain. NOL post-intubation (42.8 (31.8–50.6) vs. 34.8 (25.6–41.3), p = 0.05), median NOL during surgery (13 (11–15) vs. 11 (8–13), p = 0.027), percentage of surgical time spent with NOL > 25 (23% (18–18) vs. 20% (15–24), p = 0.036), NOL TWA < 10 (2.54 (2.1–3.0) vs. 2.86 (2.48–3.62), p = 0.044) and percentage of surgical time spent with NOL < 10 (41% (36–47) vs. 47% (40–55), p = 0.022) were associated with moderate to severe PACU pain. Corresponding ROC AUC for the prediction of moderate to severe PACU pain were 0.65 [0.51–0.79], 0.66 [0.52–0.81], 0.66 [0.52–0.79], 0.65 [0.51–0.79] and 0.67 [0.53–0.81]. Penalized logistic regression achieved the best performance with a 0.753 (0.718–0.788) CV-AUC. Our results, even if limited by the small number of patients, suggest that acute postoperative pain is better predicted by a multivariate machine-learning algorithm rather than individual intraoperative nociception variables. Further larger multicentric trials are highly recommended to better understand the relationship between intraoperative nociception and acute postoperative pain.
Trial registration Registered on ClinicalTrials.gov in October 2018 (NCT03776838).
中文翻译:
基于术中伤害感受水平 (NOL) 指数值预测术后急性疼痛:基于机器学习的分析的影响
术中伤害感受与术后急性疼痛之间的关系仍未确定。伤害感受水平 (NOL) 指数(Medasense,拉马特甘,以色列)使用多参数方法提供 0-100 的伤害感受分数。NOLGYN 研究的辅助分析的目的是评估机器学习算法根据术中 NOL 值预测中度至重度急性术后疼痛的能力。我们的研究使用来自 NOLGYN 研究的数据,这是一项随机对照试验,评估了与标准护理相比,NOL 指导的术中芬太尼给药对整体芬太尼消耗量的影响。计划进行妇科腹腔镜手术的 70 名患者(ASA I-III 级,年龄 18-75 岁)被纳入。变量包括基线人口统计数据,NOL 对切口或插管的反应、手术过程中的 NOL 中位数、高于或低于制造商推荐阈值 (10–25) 的 NOL 时间加权平均值 (TWA),以及 NOL > 25 或 < 10 的手术时间百分比。我们评估了不同的预测术后疼痛的机器学习算法。使用 ROC 曲线下的交叉验证面积 (CV-AUC) 评估性能。在分析的 66 名患者中,42 名 (63.6%) 经历了中度至重度疼痛。插管后 NOL(42.8 (31.8–50.6) 与 34.8 (25.6–41.3),p = 0.05),手术期间的 NOL 中位数(13 (11–15) 与 11 (8–13),p = 0.027), NOL > 25 的手术时间百分比(23% (18–18) 对比 20% (15–24),p = 0.036),NOL TWA < 10 (2.54 (2.1–3.0) 对比 2.86 (2.48–3.62) ), p = 0.044) 和 NOL < 10 的手术时间百分比 (41% (36–47) 对 47% (40–55), p = 0。022) 与中度至重度 PACU 疼痛有关。预测中度至重度 PACU 疼痛的相应 ROC AUC 为 0.65 [0.51–0.79]、0.66 [0.52–0.81]、0.66 [0.52–0.79]、0.65 [0.51–0.79] 和 0.67 [0.53–0.81]。惩罚逻辑回归以 0.753 (0.718–0.788) CV-AUC 实现最佳性能。我们的结果,即使受到少数患者的限制,也表明通过多变量机器学习算法而不是单个术中伤害感受变量可以更好地预测急性术后疼痛。强烈建议进行更大规模的多中心试验,以更好地了解术中伤害感受与术后急性疼痛之间的关系。66 [0.52–0.81]、0.66 [0.52–0.79]、0.65 [0.51–0.79] 和 0.67 [0.53–0.81]。惩罚逻辑回归以 0.753 (0.718–0.788) CV-AUC 实现最佳性能。我们的结果,即使受到少数患者的限制,也表明通过多变量机器学习算法而不是单个术中伤害感受变量可以更好地预测急性术后疼痛。强烈建议进行更大规模的多中心试验,以更好地了解术中伤害感受与术后急性疼痛之间的关系。66 [0.52–0.81]、0.66 [0.52–0.79]、0.65 [0.51–0.79] 和 0.67 [0.53–0.81]。惩罚逻辑回归以 0.753 (0.718–0.788) CV-AUC 实现最佳性能。我们的结果,即使受到少数患者的限制,也表明通过多变量机器学习算法而不是单个术中伤害感受变量可以更好地预测急性术后疼痛。强烈建议进行更大规模的多中心试验,以更好地了解术中伤害感受与术后急性疼痛之间的关系。表明通过多变量机器学习算法而不是单个术中伤害感受变量可以更好地预测急性术后疼痛。强烈建议进行更大规模的多中心试验,以更好地了解术中伤害感受与术后急性疼痛之间的关系。表明通过多变量机器学习算法而不是单个术中伤害感受变量可以更好地预测急性术后疼痛。强烈建议进行更大规模的多中心试验,以更好地了解术中伤害感受与术后急性疼痛之间的关系。
试验注册于 2018 年 10 月在 ClinicalTrials.gov 注册(NCT03776838)。










































 京公网安备 11010802027423号
京公网安备 11010802027423号