Annals of Intensive Care ( IF 5.7 ) Pub Date : 2022-08-02 , DOI: 10.1186/s13613-022-01039-z Charlotte Garret 1 , Marion Douillard 2 , Arthur David 3 , Morgane Péré 4 , Lucille Quenehervé 5 , Ludivine Legros 6 , Isabelle Archambeaud 2 , Frédéric Douane 3 , Marc Lerhun 2 , Nicolas Regenet 2 , Jerome Gournay 2 , Emmanuel Coron 2 , Eric Frampas 3 , Jean Reignier 1
|
Background
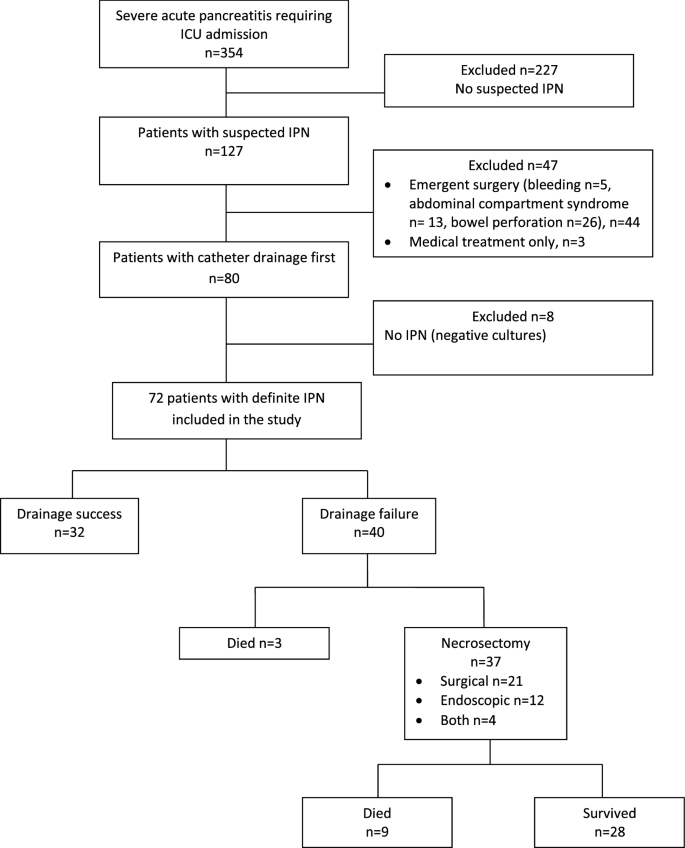
Recent guidelines advocate a step-up approach for managing suspected infected pancreatic necrosis (IPN) during acute pancreatitis. Nearly half the patients require secondary necrosectomy after catheter drainage. Our primary objective was to assess the external validity of a previously reported nomogram for catheter drainage, based on four predictors of failure. Our secondary objectives were to identify other potential predictors of catheter-drainage failure. We retrospectively studied consecutive patients admitted to the intensive care units (ICUs) of three university hospitals in France between 2012 and 2016, for severe acute pancreatitis with suspected IPN requiring catheter drainage. We assessed drainage success and failure rates in 72 patients, with success defined as survival without subsequent necrosectomy and failure as death and/or subsequent necrosectomy required by inadequate improvement. We plotted the receiver operating characteristics (ROC) curve for the nomogram and computed the area under the curve (AUROC).
Results
Catheter drainage alone was successful in 32 (44.4%) patients. The nomogram predicted catheter-drainage failure with an AUROC of 0.71. By multivariate analysis, catheter-drainage failure was independently associated with a higher body mass index [odds ratio (OR), 1.12; 95% confidence interval (95% CI), 1.00–1.24; P = 0.048], heterogeneous collection (OR, 16.7; 95% CI, 1.83–152.46; P = 0.01), and respiratory failure onset within 24 h before catheter drainage (OR, 18.34; 95% CI, 2.18–154.3; P = 0.007).
Conclusion
Over half the patients required necrosectomy after failed catheter drainage. Newly identified predictors of catheter-drainage failure were heterogeneous collection and respiratory failure. Adding these predictors to the nomogram might help to identify patients at high risk of catheter-drainage failure.
ClinicalTrials.gov number: NCT03234166.
中文翻译:
重症患者感染性胰腺坏死并发严重急性胰腺炎:预测导管引流失败和需要进行坏死组织切除术
背景
最近的指南提倡在急性胰腺炎期间管理疑似感染性胰腺坏死 (IPN) 的升级方法。近一半的患者需要在导管引流后进行二次坏死组织切除术。我们的主要目标是评估先前报道的导管引流列线图的外部有效性,基于四个失败预测因子。我们的次要目标是确定导管引流失败的其他潜在预测因素。我们回顾性研究了 2012 年至 2016 年间在法国三所大学医院的重症监护病房 (ICU) 连续收治的重症急性胰腺炎患者,疑似 IPN 需要导管引流。我们评估了 72 名患者的引流成功率和失败率,成功定义为没有后续坏死切除的存活,失败定义为死亡和/或由于改善不足而需要后续的坏死切除。我们绘制了列线图的受试者工作特征 (ROC) 曲线并计算了曲线下面积 (AUROC)。
结果
32 例 (44.4%) 患者仅导管引流成功。列线图预测导管引流失败,AUROC 为 0.71。通过多变量分析,导管引流失败与较高的体重指数独立相关[优势比 (OR),1.12;95% 置信区间 (95% CI), 1.00–1.24; P = 0.048],异质收集(OR,16.7;95% CI,1.83–152.46;P = 0.01),以及导管引流前 24 小时内出现呼吸衰竭(OR,18.34;95% CI,2.18–154.3;P = 0.007)。
结论
超过一半的患者在导管引流失败后需要进行坏死组织切除术。新发现的导管引流失败的预测因素是异质收集和呼吸衰竭。将这些预测因子添加到列线图中可能有助于识别导管引流失败高风险的患者。
ClinicalTrials.gov 编号:NCT03234166。










































 京公网安备 11010802027423号
京公网安备 11010802027423号