JACC: Cardiovascular Interventions ( IF 11.7 ) Pub Date : 2022-07-18 , DOI: 10.1016/j.jcin.2022.06.007 Bahadir Simsek 1 , Spyridon Kostantinis 1 , Judit Karacsonyi 1 , Khaldoon Alaswad 2 , Oleg Krestyaninov 3 , Dmitrii Khelimskii 3 , Rhian Davies 4 , Jeremy Rier 4 , Omer Goktekin 5 , Sevket Gorgulu 6 , Ahmed ElGuindy 7 , Raj H Chandwaney 8 , Mitul Patel 9 , Nidal Abi Rafeh 10 , Dimitrios Karmpaliotis 11 , Amirali Masoumi 11 , Jaikirshan J Khatri 12 , Farouc A Jaffer 13 , Darshan Doshi 13 , Paul B Poommipanit 14 , Bavana V Rangan 1 , Yader Sanvodal 15 , James W Choi 16 , Basem Elbarouni 17 , William Nicholson 18 , Wissam A Jaber 18 , Stephane Rinfret 18 , Michael Koutouzis 19 , Ioannis Tsiafoutis 19 , Robert W Yeh 20 , M Nicholas Burke 1 , Salman Allana 1 , Olga C Mastrodemos 1 , Emmanouil S Brilakis 1
|
Background
Chronic total occlusion (CTO) percutaneous coronary intervention (PCI) is associated with increased risk of periprocedural complications. Estimating the risk of complications facilitates risk-benefit assessment and procedural planning.
Objectives
This study sought to develop risk scores for in-hospital major adverse cardiovascular events (MACE), mortality, pericardiocentesis, and acute myocardial infarction (MI) in patients undergoing CTO PCI.
Methods
The study analyzed the PROGRESS-CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention; NCT02061436) and created risk scores for MACE, mortality, pericardiocentesis, and acute MI. Logistic regression prediction modeling was used to identify independently associated variables, and models were internally validated with bootstrapping.
Results
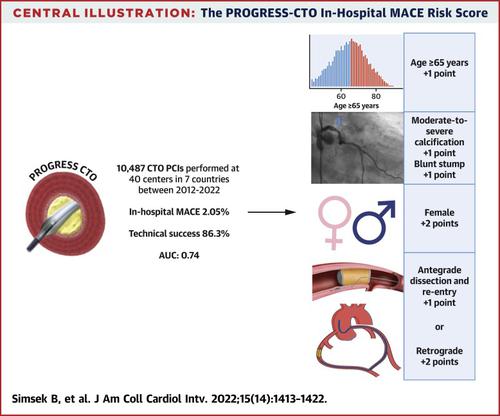
The incidence of periprocedural complications among 10,480 CTO PCIs was as follows: MACE 215 (2.05%), mortality 47 (0.45%), pericardiocentesis 83 (1.08%), and acute MI 66 (0.63%). The final model for MACE included ≥65 years of age (1 point), moderate-severe calcification (1 point), blunt stump (1 point), antegrade dissection and re-entry (ADR) (1 point), female (2 points), and retrograde (2 points); the final model for mortality included ≥65 years of age (1 point), left ventricular ejection fraction ≤45% (1 point), moderate-severe calcification (1 point), ADR (1 point), and retrograde (1 point); the final model for pericardiocentesis included ≥65 years of age (1 point), female (1 point), moderate-severe calcification (1 point), ADR (1 point), and retrograde (2 points); the final model for acute MI included prior coronary artery bypass graft surgery (1 point), atrial fibrillation (1 point), and blunt stump (1 point). The C-statistics of the models were 0.74, 0.80, 0.78, 0.72 for MACE, mortality, pericardiocentesis, and acute MI, respectively.
Conclusions
The PROGRESS-CTO complication risk scores can facilitate estimation of the periprocedural complication risk in patients undergoing CTO PCI.
中文翻译:
预测慢性完全闭塞经皮冠状动脉介入治疗的围手术期并发症
背景
慢性完全闭塞 (CTO) 经皮冠状动脉介入治疗 (PCI) 与围手术期并发症的风险增加有关。估计并发症的风险有助于风险收益评估和程序规划。
目标
本研究旨在为接受 CTO PCI 的患者制定院内主要不良心血管事件 (MACE)、死亡率、心包穿刺术和急性心肌梗死 (MI) 的风险评分。
方法
该研究分析了 PROGRESS-CTO(慢性完全闭塞干预研究的前瞻性全球登记处;NCT02061436)并创建了 MACE、死亡率、心包穿刺术和急性 MI 的风险评分。使用逻辑回归预测模型来识别独立相关变量,并使用引导程序对模型进行内部验证。
结果
10,480 例 CTO PCI 围手术期并发症的发生率如下:MACE 215 例(2.05%),死亡率 47 例(0.45%),心包穿刺 83 例(1.08%),急性心梗 66 例(0.63%)。MACE 的最终模型包括≥65 岁(1 分)、中度至重度钙化(1 分)、钝残端(1 分)、顺行剥离和再入(ADR)(1 分)、女性(2 分) ), 和逆行 (2 分); 最终的死亡率模型包括年龄≥65 岁(1 分)、左心室射血分数≤45%(1 分)、中重度钙化(1 分)、ADR(1 分)和逆行(1 分);最终的心包穿刺模型包括≥65岁(1分)、女性(1分)、中重度钙化(1分)、ADR(1分)和逆行(2分);急性 MI 的最终模型包括既往冠状动脉旁路移植术(1 分)、房颤(1 分)和钝性残肢(1 分)。模型的 MACE、死亡率、心包穿刺术和急性 MI 的 C 统计量分别为 0.74、0.80、0.78、0.72。
结论
PROGRESS-CTO 并发症风险评分有助于评估接受 CTO PCI 的患者的围手术期并发症风险。










































 京公网安备 11010802027423号
京公网安备 11010802027423号