JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2022-07-13 , DOI: 10.1016/j.jcmg.2022.05.006 Pimprapa Vejpongsa 1 , Jiaqiong Xu 2 , Miguel A Quinones 1 , Dipan J Shah 1 , William A Zoghbi 1
|
Background
Grading of aortic regurgitation (AR) and mitral regurgitation (MR) is similar in the cardiology guidelines despite distinct differences in left ventricular (LV) adaptive pathophysiology.
Objectives
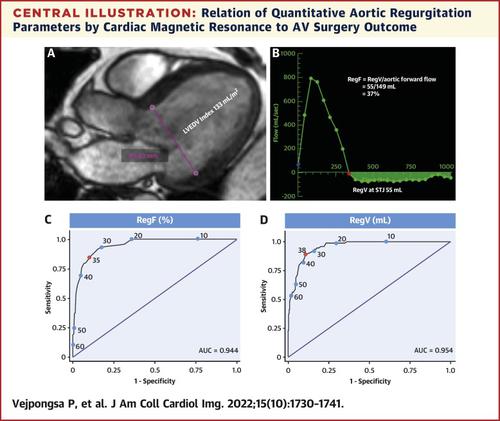
This study compared differences in LV remodeling in patients with similar degrees of AR and MR severity and evaluated optimal cutoffs for significant AR in relation to the outcome of aortic valve replacement or repair (AVR) during follow-up.
Methods
From 2008 to 2018, consecutive patients with isolated AR or MR who had cardiac magnetic resonance (CMR) were identified and CMR parameters were compared. Patients with left ventricular ejection fraction (LVEF) <50%, ischemic scar >5%, valve stenosis, or concomitant regurgitation were excluded. Patients were followed longitudinally for AVR.
Results
Baseline characteristics of isolated AR (n = 418) and isolated MR (n = 1,073) were comparable except for higher male proportion and hypertension in AR, while heart failure was more prevalent in MR. Indexed LV end-diastolic and end-systolic volumes and mass were higher in AR compared with MR at the same level of regurgitant fraction. During follow-up (mean 2.1 years), 18.7% of AR patients underwent AVR based on symptoms or LV remodeling. Interestingly, 38.0% of patients that underwent AVR within 3 months after CMR did not meet severe AVR by current guidelines of AR severity. AR regurgitant fraction>35% had high sensitivity (86%) and specificity (88%) for identifying patients who underwent AVR.
Conclusions
For similar regurgitation severity, LV remodeling is different in AR compared with MR. Cardiac symptoms and significant LV remodeling in AR requiring AVR occur frequently in patients with less severity than currently proposed. The study findings suggest that the optimal threshold for severe AR with CMR is different than MR and is lower than currently stated in the guidelines.
中文翻译:
左侧瓣膜返流中心脏重塑的差异
背景
尽管左心室 (LV) 适应性病理生理学存在明显差异,但主动脉瓣关闭不全 (AR) 和二尖瓣关闭不全 (MR) 的分级在心脏病学指南中是相似的。
目标
本研究比较了 AR 和 MR 严重程度相似的患者 LV 重塑的差异,并评估了与随访期间主动脉瓣置换或修复 (AVR) 结果相关的显着 AR 的最佳截止值。
方法
从 2008 年到 2018 年,连续确定了患有心脏磁共振 (CMR) 的孤立性 AR 或 MR 患者,并比较了 CMR 参数。左心室射血分数 (LVEF) <50%、缺血性瘢痕 >5%、瓣膜狭窄或伴随反流的患者被排除在外。对患者进行 AVR 纵向跟踪。
结果
孤立性 AR (n = 418) 和孤立性 MR (n = 1,073) 的基线特征具有可比性,除了 AR 中男性比例较高和高血压,而 MR 中心力衰竭更为普遍。在相同水平的反流分数下,AR 中的指数 LV 舒张末期和收缩末期体积和质量高于 MR。在随访期间(平均 2.1 年),18.7% 的 AR 患者根据症状或 LV 重塑接受了 AVR。有趣的是,在 CMR 后 3 个月内接受 AVR 的患者中,有 38.0% 的患者未达到当前 AR 严重程度指南的严重 AVR。AR 反流分数>35% 对识别接受 AVR 的患者具有高敏感性 (86%) 和特异性 (88%)。
结论
对于相似的反流严重程度,与 MR 相比,AR 的 LV 重塑是不同的。需要 AVR 的 AR 中的心脏症状和显着的 LV 重塑经常发生在严重程度低于目前建议的患者中。研究结果表明,CMR 严重 AR 的最佳阈值与 MR 不同,并且低于指南中目前规定的阈值。










































 京公网安备 11010802027423号
京公网安备 11010802027423号