Intensive Care Medicine ( IF 27.1 ) Pub Date : 2022-07-13 , DOI: 10.1007/s00134-022-06794-y Alexandre Mansour 1, 2, 3 , Erwan Flecher 4 , Matthieu Schmidt 5, 6 , Bertrand Rozec 7, 8 , Isabelle Gouin-Thibault 2, 9 , Maxime Esvan 10, 11 , Claire Fougerou 10, 11 , Bruno Levy 12, 13, 14 , Alizée Porto 15 , James T Ross 16 , Marylou Para 17, 18 , Sabrina Manganiello 19 , Guillaume Lebreton 6, 20 , André Vincentelli 19, 21 , Nicolas Nesseler 1, 2, 22 ,
|
Purpose
To describe bleeding and thrombotic events and their risk factors in patients receiving extracorporeal membrane oxygenation (ECMO) for severe coronavirus disease 2019 (COVID-19) and to evaluate their impact on in-hospital mortality.
Methods
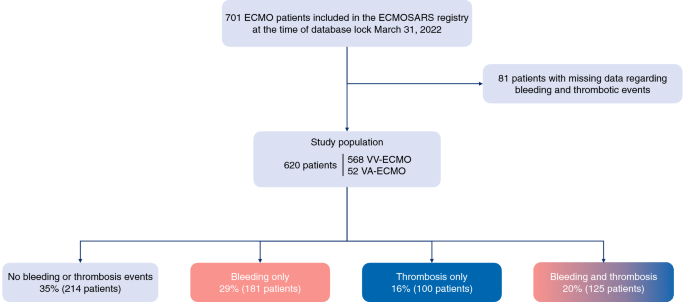
The ECMOSARS registry included COVID-19 patients supported by ECMO in France. We analyzed all patients included up to March 31, 2022 without missing data regarding bleeding and thrombotic events. The association of bleeding and thrombotic events with in-hospital mortality and pre-ECMO variables was assessed using multivariable logistic regression models.
Results
Among 620 patients supported by ECMO, 29% had only bleeding events, 16% only thrombotic events and 20% both bleeding and thrombosis. Cannulation site (18% of patients), ear nose and throat (12%), pulmonary bleeding (9%) and intracranial hemorrhage (8%) were the most frequent bleeding types. Device-related thrombosis and pulmonary embolism/thrombosis accounted for most of thrombotic events. In-hospital mortality was 55.7%. Bleeding events were associated with in-hospital mortality (adjusted odds ratio (adjOR) = 2.91[1.94–4.4]) but not thrombotic events (adjOR = 1.02[0.68–1.53]). Intracranial hemorrhage was strongly associated with in-hospital mortality (adjOR = 13.5[4.4–41.5]). Ventilation duration before ECMO ≥ 7 days and length of ECMO support were associated with bleeding. Thrombosis-associated factors were fibrinogen ≥ 6 g/L and length of ECMO support.
Conclusions
In a nationwide cohort of COVID-19 patients supported by ECMO, bleeding incidence was high and associated with mortality. Intracranial hemorrhage incidence was higher than reported for non-COVID patients and carried the highest risk of death. Thrombotic events were less frequent and not associated with mortality. Length of ECMO support was associated with a higher risk of both bleeding and thrombosis, supporting the development of strategies to minimize ECMO duration.
中文翻译:
体外膜肺氧合支持的重症 COVID-19 患者的出血和血栓事件:一项全国性队列研究
目的
描述因严重冠状病毒病 2019 (COVID-19) 接受体外膜肺氧合 (ECMO) 的患者的出血和血栓事件及其危险因素,并评估其对住院死亡率的影响。
方法
ECMOSARS 登记包括法国 ECMO 支持的 COVID-19 患者。我们分析了截至 2022 年 3 月 31 日的所有患者,没有丢失有关出血和血栓事件的数据。使用多变量逻辑回归模型评估出血和血栓事件与住院死亡率和 ECMO 前变量之间的关联。
结果
在 ECMO 支持的 620 名患者中,29% 仅发生出血事件,16% 仅发生血栓事件,20% 发生出血和血栓形成。插管部位(18% 的患者)、耳鼻喉(12%)、肺出血(9%)和颅内出血(8%)是最常见的出血类型。与器械相关的血栓形成和肺栓塞/血栓形成占血栓事件的大部分。住院死亡率为55.7%。出血事件与住院死亡率相关(调整优势比 (adjOR) = 2.91[1.94–4.4]),但与血栓事件无关(adjOR = 1.02[0.68–1.53])。颅内出血与住院死亡率密切相关(adjOR = 13.5[4.4-41.5])。ECMO ≥ 7 天前的通气时间和 ECMO 支持的时间与出血相关。
结论
在 ECMO 支持的全国 COVID-19 患者队列中,出血发生率很高并且与死亡率相关。非COVID患者的颅内出血发生率高于报道的,死亡风险最高。血栓事件发生率较低,且与死亡率无关。ECMO支持的时间与较高的出血和血栓形成风险相关,支持制定策略以最小化ECMO持续时间。










































 京公网安备 11010802027423号
京公网安备 11010802027423号