Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2022-07-11 , DOI: 10.1016/j.jacc.2022.04.049 Navin K Kapur 1 , Manreet Kanwar 2 , Shashank S Sinha 3 , Katherine L Thayer 1 , A Reshad Garan 4 , Jaime Hernandez-Montfort 5 , Yijing Zhang 1 , Borui Li 1 , Paulina Baca 1 , Fatou Dieng 1 , Neil M Harwani 1 , Jacob Abraham 6 , Gavin Hickey 7 , Sandeep Nathan 8 , Detlef Wencker 9 , Shelley Hall 9 , Andrew Schwartzman 10 , Wissam Khalife 11 , Song Li 12 , Claudius Mahr 12 , Ju H Kim 13 , Esther Vorovich 14 , Evan H Whitehead 15 , Vanessa Blumer 16 , Daniel Burkhoff 17
|
Background
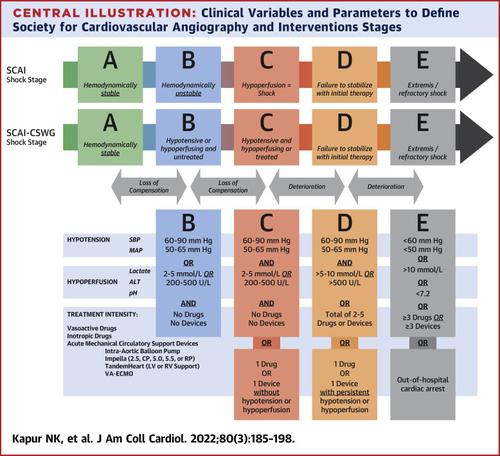
Risk-stratifying patients with cardiogenic shock (CS) is a major unmet need. The recently proposed Society for Cardiovascular Angiography and Interventions (SCAI) staging system for CS severity lacks uniform criteria defining each stage.
Objectives
The purpose of this study was to test parameters that define SCAI stages and explore their utility as predictors of in-hospital mortality in CS.
Methods
The CS Working Group registry includes patients from 17 hospitals enrolled between 2016 and 2021 and was used to define clinical profiles for CS. We selected parameters of hypotension and hypoperfusion and treatment intensity, confirmed their association with mortality, then defined formal criteria for each stage and tested the association between both baseline and maximum Stage and mortality.
Results
Of 3,455 patients, CS was caused by heart failure (52%) or myocardial infarction (32%). Mortality was 35% for the total cohort and higher among patients with myocardial infarction, out-of-hospital cardiac arrest, and treatment with increasing numbers of drugs and devices. Systolic blood pressure, lactate level, alanine transaminase level, and systemic pH were significantly associated with mortality and used to define each stage. Using these criteria, baseline and maximum stages were significantly associated with mortality (n = 1,890). Lower baseline stage was associated with a higher incidence of stage escalation and a shorter duration of time to reach maximum stage.
Conclusions
We report a novel approach to define SCAI stages and identify a significant association between baseline and maximum stage and mortality. This approach may improve clinical application of the staging system and provides new insight into the trajectory of hospitalized CS patients. (Cardiogenic Shock Working Group Registry [CSWG]; NCT04682483)
中文翻译:
定义心源性休克严重程度阶段的标准
背景
对心源性休克 (CS) 患者进行风险分层是一个主要未满足的需求。最近提出的针对 CS 严重程度的心血管造影和干预协会 (SCAI) 分期系统缺乏定义每个阶段的统一标准。
目标
本研究的目的是测试定义 SCAI 阶段的参数,并探索它们作为 CS 院内死亡率预测因子的效用。
方法
CS 工作组登记包括 2016 年至 2021 年间登记的来自 17 家医院的患者,用于定义 CS 的临床概况。我们选择了低血压和低灌注以及治疗强度的参数,确认了它们与死亡率的关联,然后为每个阶段定义了正式标准,并测试了基线和最大阶段与死亡率之间的关联。
结果
在 3,455 名患者中,CS 是由心力衰竭 (52%) 或心肌梗塞 (32%) 引起的。整个队列的死亡率为 35%,并且在患有心肌梗死、院外心脏骤停以及使用越来越多的药物和设备进行治疗的患者中死亡率更高。收缩压、乳酸水平、丙氨酸转氨酶水平和全身 pH 值与死亡率显着相关,并用于定义每个阶段。使用这些标准,基线和最大分期与死亡率显着相关 (n = 1,890)。较低的基线分期与较高的分期升级发生率和较短的达到最大分期的持续时间相关。
结论
我们报告了一种定义 SCAI 阶段的新方法,并确定了基线和最大阶段与死亡率之间的显着关联。这种方法可以改善分期系统的临床应用,并为住院 CS 患者的轨迹提供新的见解。(心源性休克工作组登记处 [CSWG];NCT04682483)










































 京公网安备 11010802027423号
京公网安备 11010802027423号