European Journal of Nuclear Medicine and Molecular Imaging ( IF 8.6 ) Pub Date : 2022-06-29 , DOI: 10.1007/s00259-022-05882-x Andrei Gafita 1, 2 , Isabel Rauscher 2 , Wolfgang P Fendler 3 , Vishnu Murthy 1 , Wang Hui 2 , Wesley R Armstrong 1 , Ken Herrmann 3 , Wolfgang A Weber 2 , Jeremie Calais 1 , Matthias Eiber 2 , Manuel Weber 3 , Matthias R Benz 1, 4
|
Purpose
To compare the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1, the adapted Prostate Cancer Working Group Criteria 3 (aPCWG3), the adapted Positron Emission Tomography Response Criteria in Solid Tumors (aPERCIST), the PSMA PET Progression (PPP), and the Response Evaluation Criteria In PSMA-Imaging (RECIP) 1.0 for response evaluation using prostate-specific membrane antigen (PSMA)-PET/CT in men with metastatic castration-resistant prostate cancer (mCRPC) treated with 177Lu-PSMA radioligand therapy.
Methods
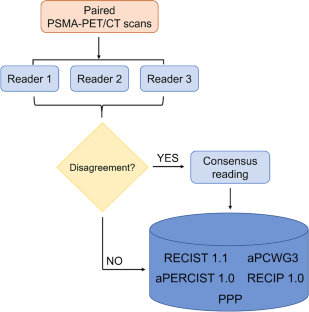
A total of 124 patients were included in this multicenter retrospective study. All patients received 177Lu-PSMA and underwent PSMA-PET/CT scans at baseline (bPET) and at 12 weeks (iPET). Imaging responses according to RECIST 1.1, aPCWG3, aPERCIST, PPP, and RECIP 1.0 were interpreted by consensus among three blinded readers. Changes in total tumor burden were obtained using the semi-automatic qPSMA software. The response according to each criterion was classified to progressive disease (PD) vs no-PD. Primary outcome measure was the prognostic value (by Cox regression analysis) for overall survival (OS). Secondary outcome measure was the inter-reader reliability (by Cohen’s κ coefficient).
Results
A total of 43 (35%) of patients had non-measurable disease according to RECIST 1.1. Sixteen (13%), 66 (52%), 72 (58%), 69 (56%), and 39 (32%) of 124 patients had PD according to RECIST 1.1, aPCWG3, aPERCIST, PPP, and RECIP, respectively. PD vs no-PD had significantly higher risk of death according to aPCWG3 (HR = 2.37; 95%CI, 1.62–3.48; p < 0.001), aPERCIST (HR = 2.48; 95%CI, 1.68–3.66; p < 0.001), PPP (HR = 2.72; 95%CI, 1.85–4.01; p < 0.001), RECIP 1.0 (HR = 4.33; 95%CI, 2.80–6.70; p < 0.001), but not according to RECIST 1.1 (HR = 1.29; 95%CI, 0.73–2.27; p = 0.38). The κ index of RECIST 1.1, aPCWG3, aPERCIST 1.0, PPP, and RECIP 1.0 for identifying PD vs no-PD were 0.50 (95%CI, 0.32–0.76), 0.72 (95%CI, 0.63–0.82), 0.68 (95%CI, 0.63–0.73), 0.73 (95%CI, 0.63–0.83), and 0.83 (95%CI, 0.77–0.88), respectively.
Conclusion
PSMA-PET-specific criteria for early response evaluation in men with mCRPC treated with 177Lu-PSMA achieved higher prognostic values and inter-reader reliabilities in comparison to conventional CT assessment or to criteria adapted to PSMA-PET from other imaging modalities. RECIP 1.0 identified the fewest patients with PD and achieved the highest risk of death for PD vs. no-PD, suggesting that other classification methods tend to overcall progression. Prospective validation of our findings on an independent patient cohort is warranted.
中文翻译:
使用 PSMA PET/CT 测量转移性去势抵抗性前列腺癌的反应:RECIST 1.1、aPCWG3、aPERCIST、PPP 和 RECIP 1.0 标准的比较
目的
比较实体瘤反应评估标准 (RECIST) 1.1、改编后的前列腺癌工作组标准 3 (aPCWG3)、改编后的实体瘤正电子发射断层扫描反应标准 (aPERCIST)、PSMA PET 进展 (PPP) 和PSMA 成像 (RECIP) 1.0 中的反应评估标准,用于使用前列腺特异性膜抗原 (PSMA)-PET/CT 对接受177 Lu-PSMA 放射配体治疗的转移性去势抵抗性前列腺癌 (mCRPC) 患者进行反应评估。
方法
这项多中心回顾性研究共纳入 124 名患者。所有患者均接受了177 Lu-PSMA,并在基线 (bPET) 和 12 周 (iPET) 时接受了 PSMA-PET/CT 扫描。根据 RECIST 1.1、aPCWG3、aPERCIST、PPP 和 RECIP 1.0 的成像反应由三位盲法读者达成共识进行解释。使用半自动 qPSMA 软件获得总肿瘤负荷的变化。根据每个标准的反应被分类为进行性疾病 (PD) 与无 PD。主要结果指标是总生存期 (OS) 的预后值(通过 Cox 回归分析)。次要结果测量是读者间的可靠性(通过 Cohen 的κ系数)。
结果
根据 RECIST 1.1,共有 43 名 (35%) 患者患有不可测量的疾病。根据 RECIST 1.1、aPCWG3、aPERCIST、PPP 和 RECIP,124 名患者中分别有 16 名 (13%)、66 名 (52%)、72 名 (58%)、69 名 (56%) 和 39 名 (32%) 患有 PD . 根据 aPCWG3(HR = 2.37;95%CI,1.62–3.48;p < 0.001),aPERCIST(HR = 2.48;95%CI,1.68–3.66;p <0.001 ),PD 与非 PD 相比具有显着更高的死亡风险, PPP (HR = 2.72; 95%CI, 1.85–4.01; p < 0.001), RECIP 1.0 (HR = 4.33; 95%CI, 2.80–6.70; p < 0.001), 但不符合 RECIST 1.1 (HR = 1.29) ;95%CI,0.73–2.27;p = 0.38)。κ _RECIST 1.1、aPCWG3、aPERCIST 1.0、PPP 和 RECIP 1.0 用于识别 PD 与无 PD 的指数分别为 0.50 (95%CI, 0.32–0.76)、0.72 (95%CI, 0.63–0.82)、0.68 (95%CI) , 0.63–0.73), 0.73 (95%CI, 0.63–0.83), 和 0.83 (95%CI, 0.77–0.88), 分别。
结论
与传统 CT 评估或适用于其他成像方式的 PSMA-PET 标准相比,使用177 Lu-PSMA治疗的 mCRPC 男性早期反应评估的 PSMA-PET 特异性标准实现了更高的预后价值和读者间可靠性。RECIP 1.0 确定的 PD 患者最少,PD 与非 PD 相比死亡风险最高,这表明其他分类方法倾向于过度调用进展。有必要对我们在独立患者队列中的发现进行前瞻性验证。










































 京公网安备 11010802027423号
京公网安备 11010802027423号