Osteoporosis International ( IF 4.2 ) Pub Date : 2022-06-24 , DOI: 10.1007/s00198-022-06462-3 M. Abdalbary , M. Sobh , S. Elnagar , M. A. Elhadedy , N. Elshabrawy , M. Abdelsalam , K. Asadipooya , A. Sabry , A. Halawa , A. El-Husseini
|
Abstract
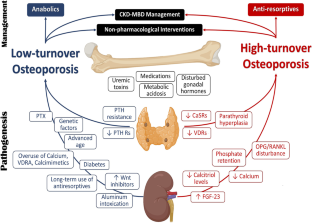
Patients with CKD have a 4–fivefold higher rate of fractures. The incidence of fractures increases with deterioration of kidney function. The process of skeletal changes in CKD patients is characterized by compromised bone strength because of deterioration of bone quantity and/or quality. The fractures lead to a deleterious effect on the quality of life and higher mortality in patients with CKD. The pathogenesis of bone loss and fracture is complex and multi-factorial. Renal osteodystrophy, uremic milieu, drugs, and systemic diseases that lead to renal failure all contribute to bone damage in CKD patients. There is no consensus on the optimal diagnostic method of compromised bone assessment in patients with CKD. Bone quantity and mass can be assessed by dual-energy x-ray absorptiometry (DXA) or quantitative computed tomography (QCT). Bone quality on the other side can be assessed by non-invasive methods such as trabecular bone score (TBS), high-resolution bone imaging methods, and invasive bone biopsy. Bone turnover markers can reflect bone remodeling, but some of them are retained by kidneys. Understanding the mechanism of bone loss is pivotal in preventing fracture in patients with CKD. Several non-pharmacological and therapeutic interventions have been reported to improve bone health. Controlling laboratory abnormalities of CKD-MBD is crucial. Anti-resorptive therapies are effective in improving BMD and reducing fracture risk, but there are uncertainties about safety and efficacy especially in advanced CKD patients. Accepting the prevalent of low bone turnover in patients with advanced CKD, the osteo-anabolics are possibly promising. Parathyroidectomy should be considered a last resort for intractable cases of renal hyperparathyroidism. There is a wide unacceptable gap in osteoporosis management in patients with CKD. This article is focusing on the updated management of CKD-MBD and osteoporosis in CKD patients.
Mini Abstract
Chronic kidney disease deteriorates bone quality and quantity. The mechanism of bone loss mainly determines pharmacological treatment. DXA and QCT provide information about bone quantity, but assessing bone quality, by TBS, high-resolution bone imaging, invasive bone biopsy, and bone turnover markers, can guide us about the mechanism of bone loss.
中文翻译:
慢性肾脏病患者骨质疏松症的管理
摘要
CKD 患者的骨折发生率高出 4-5 倍。骨折的发生率随着肾功能的恶化而增加。CKD 患者的骨骼变化过程的特征是由于骨量和/或质量的恶化导致骨强度受损。骨折对 CKD 患者的生活质量和死亡率造成有害影响。骨丢失和骨折的发病机制是复杂和多因素的。导致肾功能衰竭的肾性骨营养不良、尿毒症环境、药物和全身性疾病都会导致 CKD 患者的骨损伤。对于 CKD 患者骨受损评估的最佳诊断方法尚无共识。骨量和质量可以通过双能 X 线骨密度仪 (DXA) 或定量计算机断层扫描 (QCT) 进行评估。另一侧的骨质量可以通过非侵入性方法评估,例如骨小梁评分 (TBS)、高分辨率骨成像方法和侵入性骨活检。骨转换标志物可以反映骨重塑,但其中一些被肾脏保留。了解骨质流失的机制对于预防 CKD 患者骨折至关重要。据报道,几种非药物和治疗干预措施可以改善骨骼健康。控制 CKD-MBD 的实验室异常是至关重要的。抗骨吸收疗法可有效改善骨密度和降低骨折风险,但安全性和有效性存在不确定性,尤其是在晚期 CKD 患者中。接受晚期 CKD 患者普遍存在的低骨转换,骨合成代谢物可能很有希望。对于顽固性肾性甲状旁腺功能亢进病例,甲状旁腺切除术应被视为最后的手段。CKD 患者的骨质疏松症管理存在很大的不可接受的差距。本文重点关注 CKD-MBD 和 CKD 患者骨质疏松症的更新管理。
迷你摘要
慢性肾病会恶化骨骼的质量和数量。骨质流失的机制主要决定药物治疗。DXA 和 QCT 提供有关骨量的信息,但通过 TBS、高分辨率骨成像、侵入性骨活检和骨转换标志物评估骨质量,可以指导我们了解骨丢失的机制。










































 京公网安备 11010802027423号
京公网安备 11010802027423号