Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2022-05-23 , DOI: 10.1016/j.jacc.2022.03.367 Kathryn W Holmes 1 , Sheila Markwardt 2 , Kim A Eagle 3 , Richard B Devereux 4 , Jonathan W Weinsaft 4 , Federico M Asch 5 , Scott A LeMaire 6 , Cheryl L Maslen 7 , Howard K Song 7 , Dianna M Milewicz 8 , Siddharth K Prakash 8 , Dongchuan Guo 8 , Shaine A Morris 9 , Reed E Pyeritz 10 , Rita C Milewski 11 , William J Ravekes 12 , H C Dietz 12 , Ralph V Shohet 13 , Michael Silberbach 1 , Mary J Roman 4 ,
|
Background
The GenTAC (Genetically Triggered Thoracic Aortic Aneurysm and Cardiovascular Conditions) Registry enrolled patients with genetic aortopathies between 2007 and 2016.
Objectives
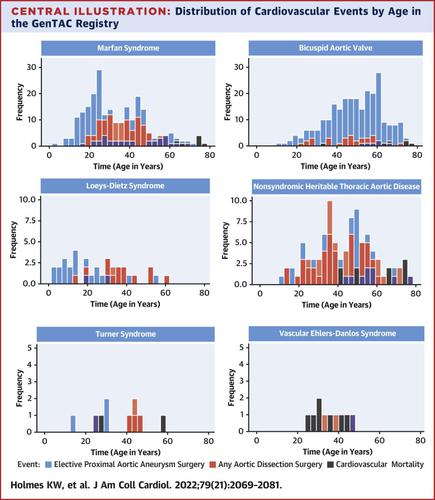
The purpose of this study was to compare age distribution and probability of elective surgery for proximal aortic aneurysm, any dissection surgery, and cardiovascular mortality among aortopathy etiologies.
Methods
The GenTAC study had a retrospective/prospective design. Participants with bicuspid aortic valve (BAV) with aneurysm (n = 879), Marfan syndrome (MFS) (n = 861), nonsyndromic heritable thoracic aortic disease (nsHTAD) (n = 378), Turner syndrome (TS) (n = 298), vascular Ehlers-Danlos syndrome (vEDS) (n = 149), and Loeys-Dietz syndrome (LDS) (n = 121) were analyzed.
Results
The 25% probability of elective proximal aortic aneurysm surgery was 30 years for LDS (95% CI: 18-37 years), followed by MFS (34 years; 95% CI: 32-36 years), nsHTAD (52 years; 95% CI: 48-56 years), and BAV (55 years; 95% CI: 53-58 years). Any dissection surgery 25% probability was highest in LDS (38 years; 95% CI: 33-53 years) followed by MFS (51 years; 95% CI: 46-57 years) and nsHTAD (54 years; 95% CI: 51-61 years). BAV experienced the largest relative frequency of elective surgery to any dissection surgery (254/33 = 7.7), compared with MFS (273/112 = 2.4), LDS (35/16 = 2.2), or nsHTAD (82/76 = 1.1). With MFS as the reference population, risk of any dissection surgery or cardiovascular mortality was lowest in BAV patients (HR: 0.13; 95% CI: 0.08-0.18; HR: 0.13; 95%: CI: 0.06-0.27, respectively). The greatest risk of mortality was seen in patients with vEDS.
Conclusions
Marfan and LDS cohorts demonstrate age and event profiles congruent with the current understanding of syndromic aortopathies. BAV events weigh toward elective replacement with relatively few dissection surgeries. Nonsyndromic HTAD patients experience near equal probability of dissection vs prophylactic surgery, possibly because of failure of early diagnosis.
中文翻译:
主动脉病的心血管结局
背景
GenTAC(基因触发的胸主动脉瘤和心血管疾病)登记处招募了 2007 年至 2016 年间患有遗传性主动脉病的患者。
目标
本研究的目的是比较主动脉病病因中近端主动脉瘤择期手术、任何夹层手术以及心血管死亡率的年龄分布和概率。
方法
GenTAC 研究采用回顾性/前瞻性设计。患有二尖瓣主动脉瓣 (BAV) 并动脉瘤 (n = 879)、马凡综合征 (MFS) (n = 861)、非综合征性遗传性胸主动脉疾病 (nsHTAD) (n = 378)、特纳综合征 (TS) (n = 298) 的参与者)、血管性 Ehlers-Danlos 综合征 (vEDS) (n = 149) 和 Loeys-Dietz 综合征 (LDS) (n = 121) 进行了分析。
结果
LDS 择期近端主动脉瘤手术的 25% 概率为 30 年(95% CI:18-37 岁),其次是 MFS(34 年;95% CI:32-36 岁)、nsHTAD(52 年;95% CI:48-56 岁)和 BAV(55 岁;95% CI:53-58 岁)。 LDS(38 岁;95% CI:33-53 岁)中任何解剖手术 25% 的概率最高,其次是 MFS(51 岁;95% CI:46-57 岁)和 nsHTAD(54 岁;95% CI:51) -61岁)。与 MFS (273/112 = 2.4)、LDS (35/16 = 2.2) 或 nsHTAD (82/76 = 1.1) 相比,BAV 的择期手术相对频率最高 (254/33 = 7.7) 。以 MFS 作为参考人群,BAV 患者发生任何解剖手术或心血管死亡的风险最低(HR:0.13;95% CI:0.08-0.18;HR:0.13;95% CI:0.06-0.27)。 vEDS 患者的死亡风险最大。
结论
Marfan 和 LDS 队列的年龄和事件概况与当前对综合征性主动脉病的理解一致。 BAV 事件倾向于选择性置换,且解剖手术相对较少。非综合征性 HTAD 患者的解剖概率与预防性手术几乎相同,这可能是因为早期诊断失败。










































 京公网安备 11010802027423号
京公网安备 11010802027423号