Annals of Intensive Care ( IF 5.7 ) Pub Date : 2022-05-16 , DOI: 10.1186/s13613-022-01012-w Hugues de Courson 1, 2 , Thomas Julien-Laferrière 1 , Delphine Georges 1 , Philippe Boyer 1 , Eric Verchère 1 , Matthieu Biais 1, 3
|
Background
Hyperoxia is associated with increased morbidity and mortality in the intensive care unit. Classical noninvasive measurements of oxygen saturation with pulse oximeters are unable to detect hyperoxia. The Oxygen Reserve Index (ORI) is a continuous noninvasive parameter provided by a multi-wave pulse oximeter that can detect hyperoxia. Primary objective was to evaluate the diagnostic accuracy of the ORI for detecting arterial oxygen tension (PaO2) > 100 mmHg in neurocritical care patients. Secondary objectives were to test the ability of ORI to detect PaO2 > 120 mmHg and the ability of pulse oximetry (SpO2) to detect PaO2 > 100 mmHg and PaO2 > 120 mmHg.
Methods
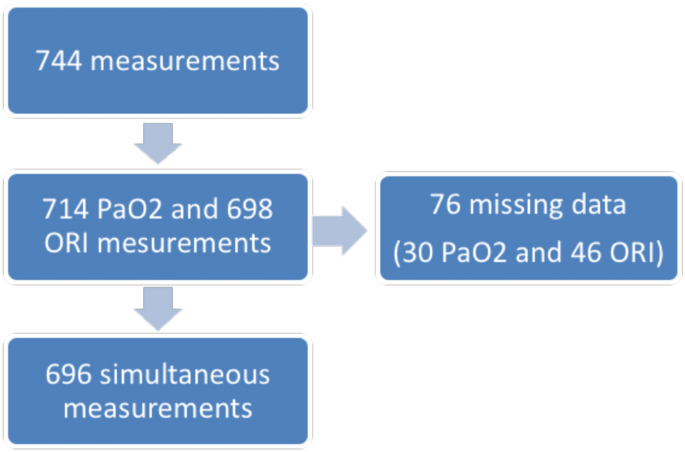
In this single-center study, we collected ORI and arterial blood samples every 6 h for 3 consecutive days. Diagnostic performance was estimated using the area under the receiver operating characteristic curve (AUROC).
Results
There were 696 simultaneous measurements of ORI and PaO2 in 62 patients. Considering the repeated measurements, the correlation between ORI and PaO2 was r = 0.13. The area under the receiver operating characteristic curve (AUROC), obtained to test the ability of ORI to detect PaO2 > 100 mmHg, was 0.567 (95% confidence interval = 0.566–0.569) with a sensitivity of 0.233 (95%CI = 0.230–0.235) and a specificity of 0.909 (95%CI = 0.907–0.910). The AUROC value obtained to test the ability of SpO2 to detect a PaO2 > 100 mmHg was 0.771 (95%CI = 0.770–0.773) with a sensitivity of 0.715 (95%CI = 0.712–0.718) and a specificity of 0.700 (95%CI = 0.697–0.703). The diagnostic performance of ORI and SpO2 for detecting PaO2 > 120 mmHg was AUROC = 0.584 (95%CI = 0.582–0.586) and 0.764 (95%CI = 0.762–0.766), respectively. The AUROC obtained for SpO2 was significantly higher than that for ORI (p < 0.01). Diagnostic performance was not affected by sedation, norepinephrine infusion, arterial partial pressure of carbon dioxide, hemoglobin level and perfusion index.
Conclusion
In a specific population of brain-injured patients hospitalized in a neurointensive care unit, our results suggest that the ability of ORI to diagnose hyperoxia is relatively low and that SpO2 provides better detection.
中文翻译:
Oxygen Reserve Index® 检测重症患者高氧的能力
背景
高氧与重症监护病房的发病率和死亡率增加有关。使用脉搏血氧仪进行氧饱和度的经典无创测量无法检测到高氧。氧储备指数 (ORI) 是由多波脉搏血氧仪提供的连续无创参数,可检测高氧。主要目的是评估 ORI 检测神经重症监护患者动脉氧分压 (PaO 2 ) > 100 mmHg 的诊断准确性。次要目标是测试 ORI 检测 PaO 2 > 120 mmHg 的能力和脉搏血氧仪 (SpO 2 ) 检测 PaO 2 > 100 mmHg 和 PaO 2 > 120 mmHg 的能力。
方法
在这项单中心研究中,我们连续 3 天每 6 小时收集一次 ORI 和动脉血样。使用受试者工作特征曲线下面积 (AUROC) 估计诊断性能。
结果
62 名患者同时进行了 696 次 ORI 和 PaO 2测量。考虑到重复测量,ORI 和 PaO 2之间的相关性为r = 0.13。为测试 ORI 检测 PaO 2 > 100 mmHg的能力而获得的受试者工作特征曲线下面积 (AUROC) 为 0.567(95% 置信区间 = 0.566–0.569),灵敏度为 0.233(95%CI = 0.230) –0.235),特异性为 0.909 (95%CI = 0.907–0.910)。获得的 AUROC 值用于测试 SpO 2检测 PaO 2的能力 > 100 mmHg 为 0.771 (95%CI = 0.770–0.773),灵敏度为 0.715 (95%CI = 0.712–0.718),特异性为 0.700 (95%CI = 0.697–0.703)。ORI 和 SpO 2检测 PaO 2 > 120 mmHg的诊断性能分别 为 AUROC = 0.584 (95%CI = 0.582–0.586) 和 0.764 (95%CI = 0.762–0.766)。SpO 2获得的 AUROC显着高于 ORI ( p < 0.01)。诊断性能不受镇静、去甲肾上腺素输注、动脉二氧化碳分压、血红蛋白水平和灌注指数的影响。
结论
在神经重症监护病房住院的特定脑损伤患者群体中,我们的结果表明 ORI 诊断高氧的能力相对较低,而 SpO 2提供了更好的检测。








































 京公网安备 11010802027423号
京公网安备 11010802027423号