Archives of Osteoporosis ( IF 3.1 ) Pub Date : 2022-05-12 , DOI: 10.1007/s11657-022-01118-5 Sarath Lekamwasam 1 , Thilina Abeygunasekara 2 , Nirmala Rathnayake 2 , Gayani Liyanage 3 , Sewwandi Subasinghe 4
|
Summary
Age-dependent upper and lower assessment thresholds help categorizing women aged 40 years or more according to their fracture risk, independent of BMD information.
Introduction
Age-dependent assessment thresholds of the FRAX algorithm help stratifying men and women aged 40 years or more according to their fracture risk. This allows clinicians to decide on those who require interventions without BMD assessment and those who require BMD input for further assessment.
Methods
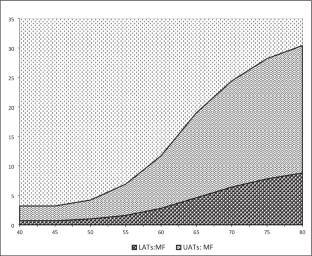
Intervention thresholds were defined by 10-year probabilities of a major osteoporotic fracture (MOF) and hip fracture (HF) considering a woman with a BMI of 25.0 kg/m2 having a prior fragility fracture but no other clinical risk factors. The lower assessment thresholds (LAT) were set at 0.8 times the 10-year probabilities of a MOF and HF in a woman with a BMI of 25.0 kg/m2, without previous fracture or other clinical risk factors. The upper assessment thresholds (UAT) were set at 1.2 times the intervention thresholds of MOF and HF. Fracture probabilities were estimated for the age range of 40–80 years, without BMD input. These values were applied to a group of women who underwent DXA for clinical reasons in a single center.
Results
The LATs of MOF and HF varied from 0.7 to 8.8% and 0.1 to 3.7%, from 40 to 80 years, respectively. The corresponding values for UATs were 2.5 to 21.6% and 0.3 to 8.4%. ITs of MOF and HF varied from 2.1 to 18% and 0.2 to 7%, respectively. When applied to a group of 315 postmenopausal women who underwent DXA for clinical indications, 22.9% of women were above the UATs (high-risk category) while 8.6% were below the LATs (low-risk category). The proportion of women in the intermediate category who require BMD for further assessment was 68.6% (95% CI 59.7 to 77.5%).
Conclusions
In nearly one-third of women aged 40 years or more, the decision to treat or not to treat can be achieved without BMD estimation. The remaining two-thirds will require a BMD assessment for further evaluation.
中文翻译:
在资源有限的环境中优化患者护理的年龄依赖性评估阈值:基于斯里兰卡 FRAX 模型的分析
概括
与年龄相关的上限和下限评估阈值有助于根据骨折风险对 40 岁或以上的女性进行分类,而不受 BMD 信息的影响。
介绍
FRAX 算法的年龄相关评估阈值有助于根据骨折风险对 40 岁或以上的男性和女性进行分层。这使临床医生可以决定哪些人需要在没有 BMD 评估的情况下进行干预,哪些人需要 BMD 输入以进行进一步评估。
方法
干预阈值定义为 10 年发生严重骨质疏松性骨折 (MOF) 和髋部骨折 (HF) 的概率,考虑 BMI 为 25.0 kg/m 2且既往有脆性骨折但没有其他临床危险因素的女性。对于 BMI 为 25.0 kg/m 2且既往没有骨折或其他临床危险因素的女性,下评估阈值 (LAT) 设定为 MOF 和 HF 10 年概率的 0.8 倍。上限评估阈值 (UAT) 设定为 MOF 和 HF 干预阈值的 1.2 倍。在没有 BMD 输入的情况下,估计了 40-80 岁年龄段的骨折概率。这些值适用于一组在单个中心因临床原因接受 DXA 的女性。
结果
从 40 年到 80 年,MOF 和 HF 的 LAT 分别从 0.7% 到 8.8% 和 0.1% 到 3.7% 不等。UAT 的相应值分别为 2.5 至 21.6% 和 0.3 至 8.4%。MOF 和 HF 的 IT 分别从 2.1% 到 18% 和 0.2% 到 7% 不等。当应用于一组 315 名因临床适应症接受 DXA 的绝经后妇女时,22.9% 的妇女高于 UAT(高风险类别),而 8.6% 低于 LAT(低风险类别)。需要进一步评估 BMD 的中间类别女性比例为 68.6%(95% CI 59.7 至 77.5%)。
结论
在将近三分之一的 40 岁或以上的女性中,可以在没有 BMD 估计的情况下做出治疗或不治疗的决定。其余三分之二将需要 BMD 评估以进行进一步评估。










































 京公网安备 11010802027423号
京公网安备 11010802027423号