JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2022-05-11 , DOI: 10.1016/j.jcmg.2022.03.017 Matthew G L Williams 1 , Kate Liang 1 , Estefania De Garate 1 , Lucrezia Spagnoli 2 , Emiliano Fiori 2 , Amardeep Dastidar 2 , Umberto Benedetto 3 , Giovanni Biglino 3 , Thomas W Johnson 2 , Thomas Luscher 4 , Chiara Bucciarelli-Ducci 5
|
Background
Patients presenting with acute coronary syndrome (ACS) and nonobstructive coronary arteries are a diagnostic dilemma. Cardiac magnetic resonance (CMR) has an overall diagnostic yield of ∼75%; however, in ∼25% of patients, CMR does not identify any myocardial injury. Identifying the underlying diagnosis has important clinical implications for patients’ management and outcome.
Objectives
The authors sought to assess whether the combination of CMR and peak troponin levels in patients with ACS and nonobstructive coronary arteries would lead to increased diagnostic yield.
Methods
Consecutive patients with ACS and nonobstructive coronary arteries without an obvious cause underwent CMR. The primary endpoint of the study was the diagnostic yield of CMR. The Youden index was used to find the optimal diagnostic cut point for peak troponin T to combine with CMR to improve diagnostic yield. Logistic or Cox regression models were used to estimate predictors of a diagnosis by CMR.
Results
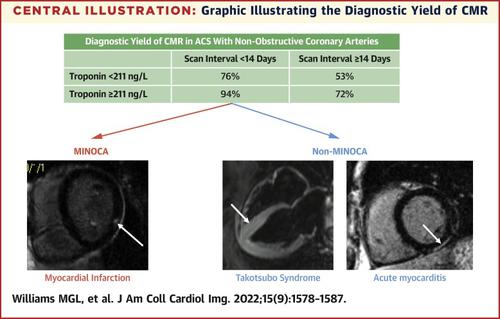
A total of 719 patients met the inclusion criteria. The peak troponin T threshold for optimal diagnostic sensitivity and specificity was 211 ng/L. Overall, CMR has a diagnostic yield of 74%. CMR performed <14 days from presentation and with a peak troponin of ≥211 ng/L (n = 198) leads to an improved diagnostic yield (94% vs 72%) compared with CMR performed ≥14 days (n = 245). When CMR was performed <14 days and with a peak troponin of <211 ng/L, the diagnostic yield was 76% (n = 86) compared with 53% (n = 190) when performed ≥14 days. An increase in 1 peak troponin decile increases the odds of the CMR identifying a diagnosis by 20% (OR: 1.20; P = 0.008, 95% CI: 1.05-1.36).
Conclusions
The combination of CMR performed <14 days from presentation and peak troponin T ≥211 ng/L leads to a very high diagnostic yield (94%) on CMR. The diagnostic yield remains high (72%) even when CMR is performed ≥14 days from presentation, but reduces to 53% when peak troponin T was <211 ng/L.
中文翻译:
峰值肌钙蛋白和 CMR 指导疑似 ACS 和非阻塞性冠状动脉的管理
背景
出现急性冠状动脉综合征 (ACS) 和非阻塞性冠状动脉的患者是一个诊断难题。心脏磁共振 (CMR) 的总体诊断率约为 75%;然而,在约 25% 的患者中,CMR 并未发现任何心肌损伤。确定潜在诊断对患者的管理和结果具有重要的临床意义。
目标
作者试图评估 ACS 和非阻塞性冠状动脉患者的 CMR 和峰值肌钙蛋白水平是否会导致诊断率增加。
方法
连续患有 ACS 和无明显原因的非阻塞性冠状动脉的患者接受了 CMR。该研究的主要终点是 CMR 的诊断率。Youden 指数用于寻找肌钙蛋白 T 峰值与 CMR 结合以提高诊断率的最佳诊断切点。Logistic 或 Cox 回归模型用于估计 CMR 诊断的预测因子。
结果
共有 719 名患者符合纳入标准。最佳诊断敏感性和特异性的峰值肌钙蛋白 T 阈值为 211 ng/L。总体而言,CMR 的诊断率为 74%。与≥14 天(n = 245)进行 CMR 相比,CMR 在出现后 14 天内进行且肌钙蛋白峰值≥211 ng/L(n = 198)可提高诊断率(94% 对 72%)。当 CMR 进行 <14 天且肌钙蛋白峰值 <211 ng/L 时,诊断率为 76%(n = 86),而进行 ≥14 天时为 53%(n = 190)。增加 1 个峰值肌钙蛋白十分位数会使 CMR 识别诊断的几率增加 20%(OR:1.20;P = 0.008,95% CI:1.05-1.36)。
结论
CMR 在出现后不到 14 天的时间和肌钙蛋白 T 峰值≥211 ng/L 的组合导致 CMR 的诊断率非常高 (94%)。即使在出现后 ≥14 天进行 CMR 时,诊断率仍然很高 (72%),但当肌钙蛋白 T 峰值 <211 ng/L 时,诊断率降至 53%。










































 京公网安备 11010802027423号
京公网安备 11010802027423号