Journal of Clinical Monitoring and Computing ( IF 2.0 ) Pub Date : 2022-05-09 , DOI: 10.1007/s10877-022-00865-7 Chao-Yuan Huang 1 , Fabian Güiza 2 , Greet De Vlieger 1, 2 , Pieter Wouters 2 , Jan Gunst 1, 2 , Michael Casaer 1, 2 , Ilse Vanhorebeek 1 , Inge Derese 1 , Greet Van den Berghe 1, 2 , Geert Meyfroidt 1, 2
|
Purpose
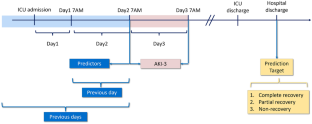
Acute kidney injury (AKI) recovery prediction remains challenging. The purpose of the present study is to develop and validate prediction models for AKI recovery at hospital discharge in critically ill patients with ICU-acquired AKI stage 3 (AKI-3).
Methods
Models were developed and validated in a development cohort (n = 229) and a matched validation cohort (n = 244) from the multicenter EPaNIC database to create prediction models with the least absolute shrinkage and selection operator (Lasso) machine-learning algorithm. We evaluated the discrimination and calibration of the models and compared their performance with plasma neutrophil gelatinase-associated lipocalin (NGAL) measured on first AKI-3 day (NGAL_AKI3) and reference model that only based on age.
Results
Complete recovery and complete or partial recovery occurred in 33.20% and 51.23% of the validation cohort patients respectively. The prediction model for complete recovery based on age, need for renal replacement therapy (RRT), diagnostic group (cardiac/surgical/trauma/others), and sepsis on admission had an area under the receiver operating characteristics curve (AUROC) of 0.53. The prediction model for complete or partial recovery based on age, need for RRT, platelet count, urea, and white blood cell count had an AUROC of 0.61. NGAL_AKI3 showed AUROCs of 0.55 and 0.53 respectively. In cardiac patients, the models had higher AUROCs of 0.60 and 0.71 than NGAL_AKI3’s AUROCs of 0.52 and 0.54. The developed models demonstrated a better performance over the reference models (only based on age) for cardiac surgery patients, but not for patients with sepsis and for a general ICU population.
Conclusion
Models to predict AKI recovery upon hospital discharge in critically ill patients with AKI-3 showed poor performance in the general ICU population, similar to the biomarker NGAL. In cardiac surgery patients, discrimination was acceptable, and better than NGAL. These findings demonstrate the difficulty of predicting non-reversible AKI early.
中文翻译:
重症成人急性肾损伤出院恢复临床预测模型的开发和验证
目的
急性肾损伤 (AKI) 恢复预测仍然具有挑战性。本研究的目的是开发和验证 ICU 获得性 AKI 3 期 (AKI-3) 危重患者出院时 AKI 恢复的预测模型。
方法
在来自多中心 EPaNIC 数据库的开发队列 (n = 229) 和匹配验证队列 (n = 244) 中开发和验证模型,以创建具有最小绝对收缩和选择算子 (Lasso) 机器学习算法的预测模型。我们评估了模型的鉴别和校准,并将它们的性能与在第一个 AKI-3 天 (NGAL_AKI3) 测量的血浆中性粒细胞明胶酶相关脂质运载蛋白 (NGAL) 和仅基于年龄的参考模型进行了比较。
结果
完全康复和完全或部分康复分别发生在 33.20% 和 51.23% 的验证队列患者中。基于年龄、肾脏替代治疗 (RRT) 需求、诊断组(心脏/手术/外伤/其他)和入院脓毒症的完全康复预测模型的受试者工作特征曲线下面积 (AUROC) 为 0.53。基于年龄、RRT 需求、血小板计数、尿素和白细胞计数的完全或部分恢复预测模型的 AUROC 为 0.61。NGAL_AKI3 显示 AUROC 分别为 0.55 和 0.53。在心脏病患者中,模型的 AUROC 为 0.60 和 0.71,高于 NGAL_AKI3 的 AUROC 0.52 和 0.54。对于心脏手术患者,开发的模型比参考模型(仅基于年龄)表现出更好的性能,
结论
预测 AKI-3 重症患者出院后 AKI 恢复的模型在一般 ICU 人群中表现不佳,类似于生物标志物 NGAL。在心脏手术患者中,歧视是可以接受的,并且优于 NGAL。这些发现证明了早期预测不可逆 AKI 的难度。










































 京公网安备 11010802027423号
京公网安备 11010802027423号