JACC: Heart Failure ( IF 10.3 ) Pub Date : 2022-05-04 , DOI: 10.1016/j.jchf.2022.02.006 Alberto Giannoni 1 , Francesco Gentile 2 , Francesco Buoncristiani 3 , Chiara Borrelli 2 , Paolo Sciarrone 2 , Jens Spiesshoefer 4 , Francesca Bramanti 3 , Giovanni Iudice 3 , Shahrokh Javaheri 5 , Michele Emdin 1 , Claudio Passino 1
|
Background
Novel treatments targeting in baroreflex sensitivity (BRS) and chemoreflex sensitivity (CRS) heart failure (HF) are grounded on small prognostic studies, partly performed in the pre–beta-blockade era.
Objectives
This study assesses the clinical/prognostic significance of BRS and CRS in a large cohort of patients with chronic HF on modern treatments.
Methods
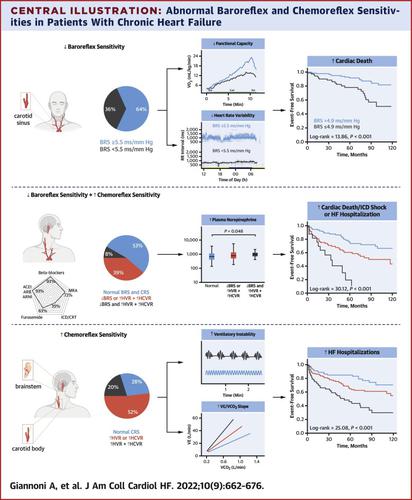
Outpatients with chronic HF with either reduced (≤40%) or mildly reduced left ventricular ejection fraction (LVEF) (41% to 49%) underwent BRS (SD method) and CRS to hypoxia and hypercapnia (rebreathing technique) assessment and were followed up for a composite endpoint of cardiac death, implantable cardioverter-defibrillator shock, or HF hospitalization.
Results
A total of 425 patients were enrolled (65 ± 12 years of age, LVEF 32% [IQR: 25%-38%], 94% on beta blockers). Patients with decreased BRS (n = 96 of 267, 36%) had lower exercise tolerance and heart rate variability (P < 0.05), whereas those with increased CRS to both hypoxia and hypercapnia (n = 74 of 369, 20%) had higher plasma norepinephrine and central apneas across the 24-hour period (P < 0.01). During a median 50-month follow-up (IQR: 24-94 months), the primary endpoint occurred more often in patients with decreased BRS (log-rank: 11.64; P = 0.001), mainly for increased cardiac deaths/implantable cardioverter-defibrillator shocks, and in those with increased CRS (log-rank: 34.81; P < 0.001), mainly for increased HF hospitalizations. Patients with both abnormal BRS and CRS showed the worst outcome. Reduced BRS (HR: 2.76 [95% CI: 1.36-5.63]; P = 0.005) and increased CRS (HR: 2.91 [95% CI: 1.34-6.31]; P = 0.007) were independently associated with the primary outcome and increased risk stratification when added to standard HF prognosticators (P < 0.05).
Conclusions
In subjects with HF on modern treatment, abnormal BRS and CRS are frequently observed. BRS and CRS elicit autonomic imbalance, exercise limitation, unstable ventilation, and predict adverse outcomes.
中文翻译:
Chemoreflex 和压力反射敏感性在慢性心力衰竭中具有很强的预后价值
背景
针对压力反射敏感性 (BRS) 和化学反射敏感性 (CRS) 心力衰竭 (HF) 的新型治疗基于小型预后研究,部分研究是在β-阻断前时代进行的。
目标
本研究评估了 BRS 和 CRS 在大量接受现代治疗的慢性 HF 患者中的临床/预后意义。
方法
左心室射血分数 (LVEF) 降低(≤40%)或轻度降低(41% 至 49%)的慢性 HF 门诊患者接受 BRS(SD 方法)和 CRS 对缺氧和高碳酸血症(再呼吸技术)的评估并进行随访用于心源性死亡、植入式心脏复律除颤器休克或心衰住院的复合终点。
结果
共有 425 名患者入组(65 ± 12 岁,LVEF 32% [IQR: 25%-38%],94% 使用 β 受体阻滞剂)。BRS 降低的患者(n = 267 中的 96 例,36%)具有较低的运动耐量和心率变异性(P < 0.05),而 CRS 升高到缺氧和高碳酸血症的患者(n = 369 中的 74 例,20%)具有更高24 小时血浆去甲肾上腺素和中枢性呼吸暂停(P < 0.01)。在中位 50 个月的随访期间(IQR:24-94 个月),主要终点更常见于 BRS 降低的患者(对数秩:11.64;P = 0.001),主要是心源性死亡/植入式心脏复律器-除颤器电击,以及 CRS 升高的患者(对数秩:34.81;P <0.001),主要是因为心衰住院人数增加。BRS和CRS都异常的患者表现出最差的结果。BRS 降低 (HR: 2.76 [95% CI: 1.36-5.63]; P = 0.005) 和 CRS 增加 (HR: 2.91 [95% CI: 1.34-6.31]; P = 0.007) 与主要结局独立相关并且增加添加到标准 HF 预测器时的风险分层(P < 0.05)。
结论
在接受现代治疗的 HF 受试者中,经常观察到异常 BRS 和 CRS。BRS 和 CRS 引起自主神经失衡、运动受限、通气不稳定并预测不良结果。








































 京公网安备 11010802027423号
京公网安备 11010802027423号