Annals of Intensive Care ( IF 5.7 ) Pub Date : 2022-04-11 , DOI: 10.1186/s13613-022-01005-9 Marie Lecronier 1, 2 , Boris Jung 3, 4 , Nicolas Molinari 5 , Jérôme Pinot 1 , Thomas Similowski 1, 2 , Samir Jaber 3, 4 , Alexandre Demoule 1, 2 , Martin Dres 1, 2
|
Background
Whether sepsis-associated diaphragm dysfunction may improve despite the exposure of mechanical ventilation in critically ill patients is unclear. This study aims at describing the diaphragm function time course of septic and non-septic mechanically ventilated patients.
Methods
Secondary analysis of two prospective observational studies of mechanically ventilated patients in whom diaphragm function was assessed twice: within the 24 h after intubation and when patients were switched to pressure support mode, by measuring the endotracheal pressure in response to bilateral anterior magnetic phrenic nerve stimulation (Ptr,stim). Change in diaphragm function was expressed as the difference between Ptr,stim measured under pressure support mode and Ptr,stim measured within the 24 h after intubation. Sepsis was defined according to the Sepsis-3 international guidelines upon inclusion. In a sub-group of patients, the right hemidiaphragm thickness was measured by ultrasound.
Results
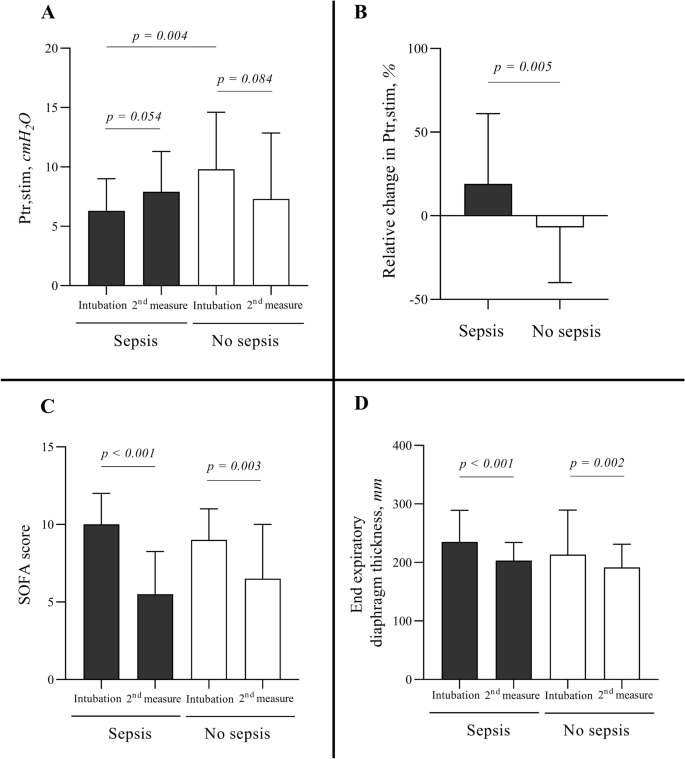
Ninety-two patients were enrolled in the study. Sepsis upon intubation was present in 51 (55%) patients. In septic patients, primary reason for ventilation was acute respiratory failure related to pneumonia (37/51; 73%). In non-septic patients, main reasons for ventilation were acute respiratory failure not related to pneumonia (16/41; 39%), coma (13/41; 32%) and cardiac arrest (6/41; 15%). Ptr,stim within 24 h after intubation was lower in septic patients as compared to non-septic patients: 6.3 (4.9–8.7) cmH2O vs. 9.8 (7.0–14.2) cmH2O (p = 0.004), respectively. The median (interquartile) duration of mechanical ventilation between first and second diaphragm evaluation was 4 (2–6) days in septic patients and 3 (2–4) days in non-septic patients (p = 0.073). Between first and second measurements, the change in Ptr,stim was + 19% (− 13–61) in septic patients and − 7% (− 40–12) in non-septic patients (p = 0.005). In the sub-group of patients with ultrasound measurements, end-expiratory diaphragm thickness decreased in both, septic and non-septic patients. The 28-day mortality was higher in patients with decrease or no change in diaphragm function.
Conclusion
Septic patients were associated with a more severe but reversible impaired diaphragm function as compared to non-septic patients. Increase in diaphragm function was associated with a better survival.
中文翻译:
脓毒症机械通气患者严重但可逆的膈肌功能受损
背景
尽管危重患者接受了机械通气,但脓毒症相关的膈肌功能障碍是否会有所改善尚不清楚。本研究旨在描述脓毒症和非脓毒症机械通气患者的膈肌功能时间过程。
方法
对机械通气患者的两项前瞻性观察性研究进行二次分析,其中两次评估膈肌功能:插管后 24 小时内和患者切换到压力支持模式时,通过测量双侧膈前神经刺激反应的气管内压力。点,刺激)。隔膜功能的变化表示为压力支持模式下测量的 Ptr,stim 与插管后 24 h 内测量的 Ptr,stim 之差。脓毒症在纳入时根据 Sepsis-3 国际指南进行定义。在一个亚组患者中,通过超声测量右侧膈肌厚度。
结果
92名患者参加了这项研究。51 名 (55%) 患者在插管时出现脓毒症。在脓毒症患者中,通气的主要原因是与肺炎相关的急性呼吸衰竭(37/51;73%)。在非脓毒症患者中,通气的主要原因是与肺炎无关的急性呼吸衰竭(16/41;39%)、昏迷(13/41;32%)和心脏骤停(6/41;15%)。与非脓毒症患者相比,脓毒症患者插管后 24 小时内的 Ptr,stim 较低:分别为 6.3 (4.9-8.7) cmH 2 O 和 9.8 (7.0-14.2) cmH 2 O ( p = 0.004)。第一次和第二次膈肌评估之间机械通气的中位(四分位数)持续时间在脓毒症患者中为 4(2-6)天,在非脓毒症患者中为 3(2-4)天(p = 0.073)。在第一次和第二次测量之间,Ptr,stim 的变化在脓毒症患者中为 + 19% (- 13-61),在非脓毒症患者中为 - 7% (- 40-12) ( p = 0.005)。在进行超声测量的患者亚组中,脓毒症和非脓毒症患者的呼气末隔膜厚度均有所降低。膈肌功能下降或无变化的患者28天死亡率较高。
结论
与非脓毒症患者相比,脓毒症患者的膈肌功能受损更严重但可逆。膈肌功能的增加与更好的生存率相关。










































 京公网安备 11010802027423号
京公网安备 11010802027423号